
Abstract
Ciprofloxacin has become the antibiotic of choice for the treatment of typhoid fever with the emergence and worldwide spread of Salmonella enterica typhi strains resistant to chloramphenicol. However, the rampant use of ciprofloxacin gradually led to an increase in its minimum inhibitory concentration against S. enterica typhi. This threatened its therapeutic efficacy and resulted in the re-emergence of chloramphenicol-sensitive S. enterica typhi strains.
Introduction
Chloramphenicol was first introduced in 1948 and became the drug of choice for typhoid fever for three decades, despite sporadic reports of resistance and the introduction of several new promising agents. Treatment with chloramphenicol reduced mortality due to typhoid fever from 20%, in the pre-antibiotic era, to 1% and decreased the duration of fever from 14–28 days to 3–5 days. However, in the early 1970s, widespread plasmid-mediated chloramphenicol resistance emerged in S. enterica typhi with outbreaks in South India, Mexico, Vietnam, Korea and Thailand. This led to the replacement of chloramphenicol by ciprofloxacin as the drug of choice. However, the rampant use of ciprofloxacin gradually led to an increase in its minimum inhibitory concentration (MIC) which threatened its therapeutic efficacy. The withdrawal of selective pressure resulted in the re-emergence of chloramphenicol susceptibility.
Methods and results
The present study was undertaken in order to study the antimicrobial susceptibility pattern of S. enterica typhi and to evaluate the efficacy of ciprofloxacin and chloramphenicol as determined by their MIC values.
Eighty-seven strains of S. enterica typhi isolated from the blood cultures of patients from January 2006 to May 2007 were included in the study. Antimicrobial susceptibility was evaluated by the Kirby-Bauer disc diffusion technique using discs of standard concentration (Himedia Laboratories Pvt Ltd, Mumbai). The MIC of ciprofloxacin and chloramphenicol was determined by the agar dilution method using Mueller-Hinton agar (Himedia Laboratories Pvt Ltd, Mumbai) according to criteria of the Clinical Laboratory Standards Institute (CLSI). 1 The concentrations of antimicrobial agents used were dilutions doubled from 0.0625 μg/mL to 32.0 μg/mL.
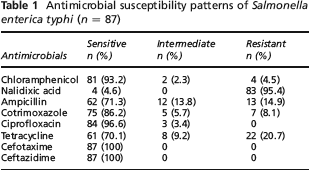
All 87 isolates were sensitive to the third generation cephalosporins, i.e. cefotaxime and ceftazidime. Sensitivity to ciprofloxacin was 84 (96.6%) and the resistance to nalidixic acid was high (83, 95.4%; see Table 1). The MIC of ciprofloxacin ranged from 0.125 μg/mL–2.0 μg/mL. Eighty-one (93.2%) strains were sensitive to chloramphenicol with MIC ≤ 8 μg/mL. Nine different antimicrobial resistance patterns were observed: 51 isolates were resistant only to nalidixic acid (N); seven to nalidixic acid and ampicillin (NA); 16 to nalidixic acid and tetracycline (NT); two to nalidixic acid, ampicillin and cotrimoxazole (NACo); one to nalidixic acid, ampicillin and tetracycline (NAT); one to nalidixic acid, tetracycline and chloramphenicol (NTC); two to nalidixic acid, tetracycline and cotrimoxazole (NTCo); one to nalidixic acid, ampicillin, cotrimoxazole and chloramphenicol (NACoC); and two to nalidixic acid, ampicillin, cotrimoxazole, chloramphenicol and tetracycline (NACoCT). Nine strains were resistant to three or more drugs. Three strains were simultaneously resistant to ampicillin, chloramphenicol and cotrimoxazole.
Antimicrobial susceptibility patterns of Salmonella enterica typhi (n = 87)
Discussion
Several Indian studies have documented a 90–95% re-emergence of chloramphenicol susceptibility. 2 A re-emergence of chloramphenicol susceptibility has also been reported from neighbouring countries. In a study conducted in Nepal, complete clinical cure without complications or relapse has been reported in 83% of patients treated with chloramphenicol. 3 A significant decrease in the isolation of chloramphenicol resistant S. enterica typhi has been reported from Bangladesh. 4
The selective pressure on the bacterial population from the uncontrolled use of quinolones has led to the emergence of a resistance to this group of antimicrobials. One mutation in the gyrA gene mediates full resistance to narrow-spectrum quinolones, such as nalidixic acid, and decreased susceptibility to fluoroquinolones. A second mutation in either the gyrA or the gyrB genes mediates full resistance to fluoroquinolones.
During 1989–1990, there were reports of fever subsiding after a mean of three days of ciprofloxacin therapy. 5 From 1993, reports appeared of fever subsiding after five to six days of treatment. 6 In one community-based study, 21.9% of cases took longer than eight days to become afebrile and 9% did not respond to ciprofloxacin even after 15 days of treatment despite in vitro susceptibility. 7 This discordance between in vitro and in vivo susceptibility was due to an increase in MIC, although according to CLSI all strains were sensitive to ciprofloxacin. In the present study, there is an increase in MIC (0.125 μg/mL–2.0 μg/mL), although there is 100% susceptibility according to the disc diffusion method. Treatment failures have been reported in patients infected with strains having an MIC of between 0.12–1 μg/mL. 8 This indicates a need to revise the current CLSI breakpoints (≤1.0 μg/mL) for ciprofloxacin susceptibility. High ciprofloxacin breakpoints not only misguide the clinicians but also affect the surveillance of resistance.
Nalidixic acid resistance is a marker of low-level resistance and treatment failure to ciprofloxacin. Nalidixic acid resistant S. enterica typhi are endemic in the Indian subcontinent. In our study the resistance to nalidixic acid was 83 (95.4%). In Vietnam up to 95% of S. enterica typhi are resistant to nalidixic acid. There is an unpredictable response to treatment with ciprofloxacin in patients infected with these kinds of isolates. Hence, nalidixic acid susceptibility testing must be included with ciprofloxacin susceptibility testing. Treatment with ciprofloxacin should be avoided in nalidixic acid resistant S. enterica typhi although higher doses may be helpful in a few cases. However, lowering susceptibility breakpoints can negate the need for the use of nalidixic acid screening test.
In the 1990s, multidrug resistance (MDR) of up to 90% was reported from India and the neighbouring countries. However, there are now reports on the decline in MDR which is possibly due to the re-emergence of chloramphenicol susceptibility. 4 In the present study only nine (10.3%) isolates were resistant to three or more drugs, and of these only three (3.4%) showed a simultaneous resistance to ampicillin, cotrimoxazole and chloramphenicol. Because of the reduced susceptibility to ciprofloxacin, third generation cephalosporins are gaining importance in the treatment of MDR typhoid fever. However, the high cost of the drugs and the need for parenteral administration are the associated disadvantages. Moreover, treatment failures have been reported in even those treated with cephalosporins. 9
Conclusion
The changing trends in the antibiograms of S. enterica typhi demand the judicious use of ciprofloxacin and a reconsideration of the use of chloramphenicol in the treatment of typhoid fever. Without this the trend towards an increasing MIC of ciprofloxacin will leave us with expensive third generation cephalosporins as our only option.
Chloramphenicol is cheaper than the third generation cephalosporins, is administered orally and its clinical efficacy well established. Where drug sensitivity tests are not available, chloramphenicol can be given in uncomplicated typhoid fever and the response monitored carefully. If fever subsides within five days the drug must be continued. Otherwise, if the temperature does not become normal within seven days, one should resort to ciprofloxacin therapy. In complicated cases, or patients in whom diagnosis and therapy had been delayed beyond two weeks, there may be justification for the institution of ciprofloxacin therapy. 10