
Abstract
A coin in the oesophagus is a common paediatric emergency in Zambia. There are very few specialist surgeons and hospitals where endoscopic removal can be carried out in many resource-limited countries. The technique described here allows the removal of an ingested coin using an ordinary Foley's catheter. The use of this technique under fluoroscopic guidance has been described in literature. However, fluoroscopic facilities and trained radiologists are not commonly available in many parts of Africa. This technique is simple, safe and has a success rate close to that achieved by endoscopic removal.
Introduction
A common paediatric emergency seen in Zambia is that of a child with a foreign body in the oesophagus. 1 Usually the foreign body is a coin. Zambia has 72 district hospitals and only four specialist hospitals. 2 There is only one paediatric surgical centre with paediatric endoscopy facilities and there are only 40 registered surgical specialists. 3 Therefore, the vast majority of children presenting with this condition will neither have access to a specialist nor to the specialist equipment required to remove a swallowed coin. Little et al. described the use of Foley's catheter under fluoroscopic guidance. 4 However, fluoroscopy is not commonly available in many of the district hospitals in Zambia.
This situation is common in many of the resourced-limited countries in Africa and other developing countries. The World Health Organization surgical guidelines for district hospitals recommend that foreign bodies in the upper oesophageal should be removed using a laryngoscope and Magills forceps. It recommends endoscopic removal for all other sites. 5
We have developed a successful technique for the removal of non-sharp foreign bodies using a Foley's urinary catheter without the use of fluoroscopy.
Technique
Coins are most frequently swallowed by children under five years old. 5 The child is likely to present with dysphagia and drooling of saliva. 6 The most common anatomical site is the upper oesophagus in the cricopharngeus area. 4 The ingestion may have been observed and reported, or not observed but indicated by the symptoms. 7 A chest radiograph is required in order to confirm the diagnosis. The coin usually lies in the coronal plane because of the anatomical design of the oesophagus which, when relaxed, is collapsed and has a wider lateral diameter than the anterior posterior plane. The coin may occasionally lie in the saggital plane, in which case a lateral chest X-ray is necessary. 8 A non-symptomatic coin maybe left alone until it has been passed, but a symptomatic coin, or a coin that is static in the oesophagus, requires active management. 9
Step 1
The diagnosis of a swallowed coin is made on the basis of the history and a plain chest X-ray, usually a posterior anterior view is adequate (Figure 1). When the coin is symptomatic or impacted active management is advocated. Parental anxiety or social circumstances may also dictate active management.
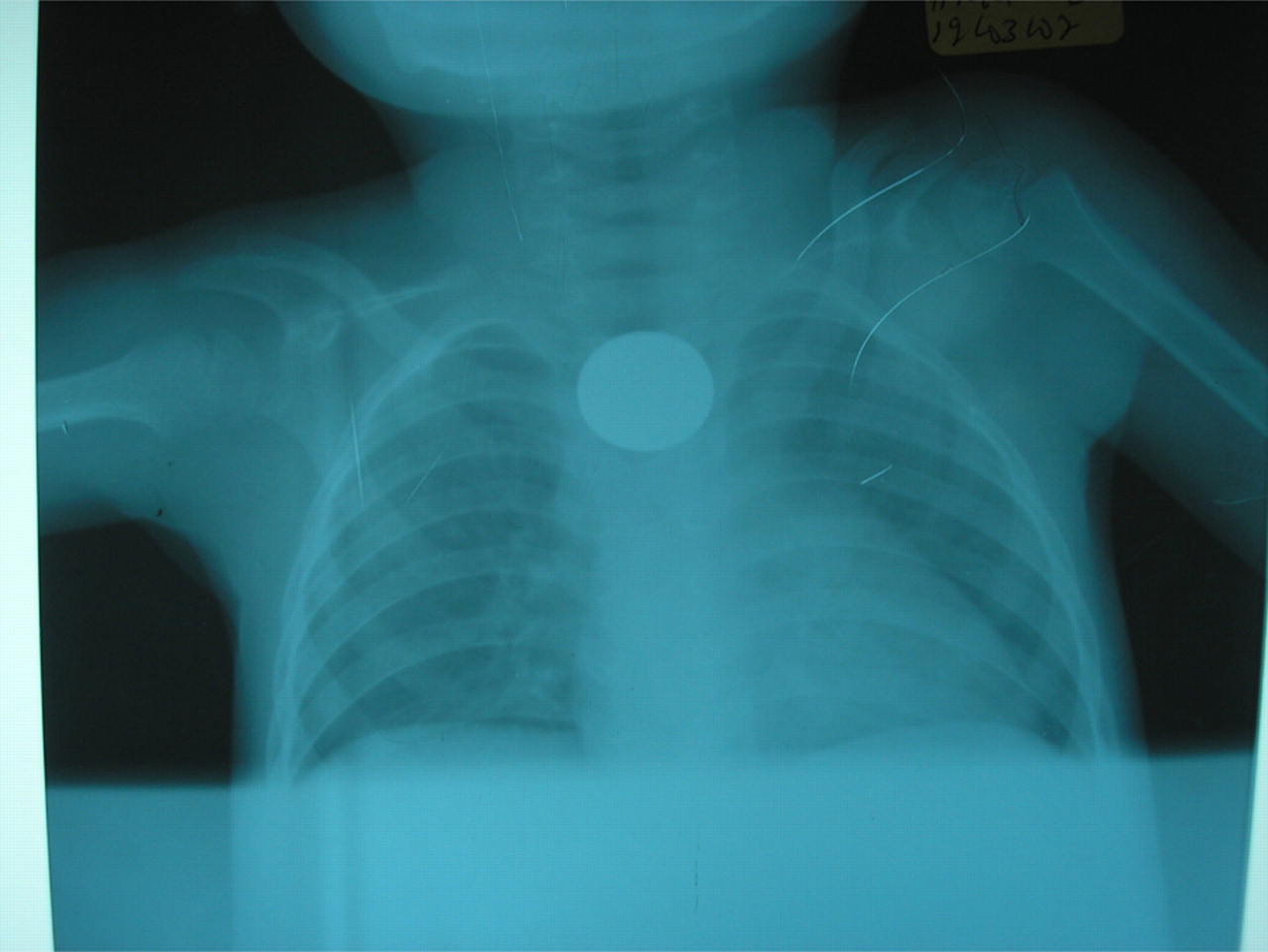
Posterior anterior chest X ray film showing a coin in the oesophagus
The child must be given general anaesthesia and intubated with a cuffed endotracheal tube. It is important to do this before making any attempt to remove the coin. If it is not done the coin may enter the trachea in the process of oesophageal extraction.
Step 2
The surgeon should be positioned at the head end of the bed, with the patient's neck rested on a sand bag, so that the head is extended on a slightly flexed neck (Figure 2). A size 16 Foley's catheter is used and lubricated with KY jelly. The catheter is inserted posteriorly behind the endotracheal tube. A long-bladed laryngoscope may be used to lift the epiglottis up in order to observe the oesophagus while inserting the catheter. The catheter will usually slide past the coin without dislodging it. If it is dislodged, the coin is likely to be pushed safely into the stomach. The catheter is pushed down as far as it can go and will usually fall just short of the stomach.

Intubation of a young boy
The catheter should then be slowly inflated with 5 mL of saline and slowly pulled up. When it meets the coin there is usually some slight resistances and gentle traction is necessary. The coin will then be seen to easily come up into the oral pharynx with an accompanying mild popping sound.
Step 3
The coin will be seen in the oral pharynx and will then be easily removed with a Magills' forcep.
Conclusion
With a team of trainee surgeons, the University Hospital team conducts once monthly mobile outreaches to district hospitals in remote country areas. During the mobile outreach the team has removed a number of swallowed coins, with a success rate of about 80% (unpublished observation).
This success rate is very close to the 85% obtained using fluoroscopic guided coin removal. 10
In our experience this technique is safe and requires minimal resources. We have not found any reports in the literature describing the use of Foley's catheter without fluoroscopy guidance.
Endoscopy technique has a reported success rate of 95%, but paediatric endoscopy equipment is not readily available in many of the resource-limited countries in Africa, in general, and Zambia in particular.