
Abstract
The classification of epilepsy, which represents the commonest neurological disorder throughout the developing world, has been difficult due to lack of diagnostic tools. Adapted to the circumstances of an epilepsy clinic in northern Tanzania, we grouped people with epilepsy (PWE) according to an adjusted version of the International Classification of Epileptic Seizures with the main groups being: generalized types of seizures (206 PWE) divided into those starting within (147 PWE) and those starting outside (59 PWE) a specific age range (6–25 years); and partial types of seizures (102 PWE) with subgroups of generalized seizures with diffuse brain damage (41 PWE), those with predominantly focal signs (60 PWE) and complex partial seizures (1 PWE). Clinical implications are discussed.
Introduction
Classifying epileptic seizures has been a challenge over the last decades. In 1981, the International League Against Epilepsy (ILAE) adopted the current International Classification of Epileptic Seizures (ICES) and in 1985, accepted the International Classification of Epilepsies, Epileptic Syndromes and Related Disorders (ICEES).1,2 Although both have been universally accepted and have proven to be of considerable clinical value, it has become clear that adjustments may be needed for specific applications such as for example epidemiological studies and resource-poor settings. To date, the ICES and ICEES have been used too loosely in studies of sub-Saharan Africa. It is not only seizure semiology, the description of which due to sociocultural barriers may be incomplete, but important seizure-related issues such as aetiology and concomitant diseases, which may be relevant for the classification of epilepsy in these countries. We have recently suggested an adapted ILAE version for epileptic seizures thought to be more appropriate for classification of epileptic seizures in sub-Saharan Africa. 3 In this study, we want to share our experience with medical doctors working with people with epilepsy (PWE) in resource-poor countries by means of analysis of over 300 PWE applying the adapted ILAE classification.
Methods
The epilepsy clinic
An epilepsy clinic, with the aim to provide specialist care to PWE, was established at Haydom Lutheran Hospital (HLH) in the northern part of Tanzania. To ensure optimum treatment without the help of specialist physicians from abroad, standardised questionnaires and guidelines were developed (www.haydom.no).
Classification
The suggested classification is based on description of seizures by the patients and at least one witness, history of seizures with special emphasis on age of onset, associated illness, family history and birth history, as well as a complete neurological examination. Electroencephalogram (EEG) and neuroimaging were not available; thus, the diagnosis is based on clinical signs and symptoms alone. Epilepsy was defined as two or more afebrile epileptic seizures unrelated to acute metabolic disorders or withdrawal of drugs or alcohol.4,5 All patients had active epilepsy.4,5 In our study, the term ‘primary generalized seizure’ as opposed to ‘secondary generalized seizure’ was used to indicate that there was no focal start of the seizure in a patient who otherwise was healthy. The classification of epileptic seizures is discussed below:
(1) Generalized types of seizures.
Generalized seizures 3 within a specific age range: primary generalized seizures that start within a specific age group (mainly between 6 and 25 years). There is no obvious cause for the seizures; brain damage is absent. However, there may be a positive family history, suggesting a possible genetic background. Seizures of this group may also be termed idiopathic generalized epilepsies.
Generalized seizures outside a specific age range: primary generalized seizures that start outside the specific age range of most of the idiopathic generalized epilepsies, but have no focal start and no clinical signs of brain damage. There may be a cause which cannot be diagnosed with the currently available ancillary means; thus, these seizures may be termed ‘cryptogenic’.
(2) Partial types of seizures.
Generalized seizures 3 with diffuse brain damage: clinically seizures start in a generalized way; however, diffuse brain damage is obvious, which is the major difference when compared to group 1. Causes are mainly due to static encephalopathies. All age groups can be affected, but there tends to be a shift to the younger ages.
Generalized seizures with focal signs: secondary generalized seizures with a focal start or clear unilateral seizures, but without major brain damage. There may be developmental delay, subtle signs of brain damage and/or focal neurology. Causes are often due to progressive encephalopathies. All age groups can be affected.
Complex partial seizures: as defined by the ILAE. 1
Simple partial seizures: as defined by the ILAE. 1
(3) Other types of seizures.
Two different seizure types: the patient has more than one type of seizure. Possible combinations are simple partial or complex partial seizures with any of the generalized seizures of group 2. Generalized seizures of group 1 and pseudoseizures are also included in this type.
Unclassified epileptic seizures: include all those seizures that cannot be classified because of incomplete data.
Ethical issues
Ethical clearance was given by the National Institute of Medical Research and the study was approved by the Tanzania Commission for Science and Technology. Informed consent was obtained.
Results
Demographics
A total number of 346 patients were seen between August 2002 and September 2004. Patients presenting to the clinic were mainly adults, with a median age of 19 years (range: one week to 80 years). The male to female ratio was 1.08.
Seizure history
Of the 346 patients registered, 337 (97.4%) were diagnosed as having genuine epilepsy. Details on diagnoses, age at presentation and gender are given in Table 1.
Classification of the seizures and demographic details

Discussion
In our study, we opted for a simple-structured, easy-to-understand classification of epileptic seizures, which is still in accordance with the ICES and in fact shares many similarities with the ILAE version of guidelines for epidemiologic studies on epilepsy (see methods).3,4 The major aim of the suggested classification is the purposeful grouping of epileptic seizures within the clinical setting, with special emphasis on further clinical work-up and treatment in a rural African hospital (Figure 1).
3
Algorithm on how to classify PWE in resource-poor countries regarding diagnostic and therapeutic implications. Primary generalized seizures were split according to the age of onset (see methods); the two groups have a different diagnostic and therapeutic approach. Patients with primary generalized seizures that start outside the range 6–25 years may have cerebral lesions and therefore need further investigation. In PWE with diffuse brain damage, diagnostic tests are rarely needed as the extent of the cerebral sequelae is known and the condition is not progressive. In contrast, in PWE who show focal signs without diffuse brain damage, further diagnostic steps are essential in order to identify the underlying, potentially treatable cause. In all four groups, treatment depends on the age of the patient, the presence of mental handicap and focal neurology, bearing in mind that the choice of antiepileptic medication is limited. CBZ, carbamazepine; CT, computerised tomography; EEG, electroencephalogram; PHB, phenobarbitone; PHT, phenytoin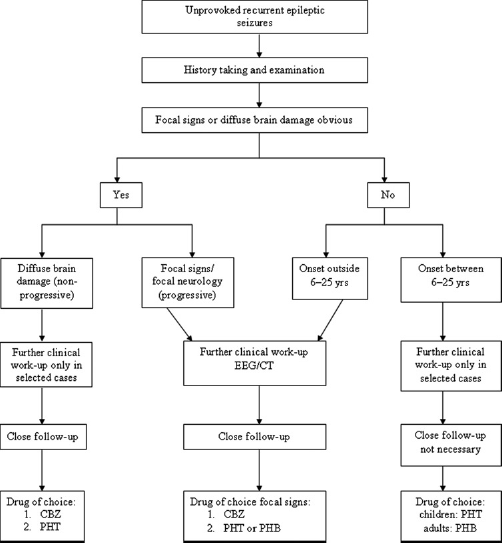
The age of our patients was similar to that in other African studies; the almost equal gender distribution, however, was atypical.6–9 This may reflect a change in gender-related access to health-care systems in our study area most likely due to information campaigns. We were able to classify most of the epilepsy cases, but five, in whom the information was incomplete. 60% belonged to the generalized epilepsies. Whether or not seizures in rural Africa are primarily generalized or focal is still controversial. Some research groups in different African countries found that primary generalized seizures were more prevalent; others, however, report more focal seizures. 10 Classification of epileptic seizures also depends on the availability of EEG and neuroimaging, which may explain the different results. In our study, these diagnostic tools were not at hand, which may have led to an overrepresentation of generalized types of epilepsy.
In summary, we present clinical data on over 300 PWE classified according to an adjusted version of the ICES for specific use in resource-poor countries (Figure 1).
Footnotes
Acknowledgements
We are very grateful to the Savoy Epilepsy Foundation, Canada, for supporting this study and to the nurses, Michaeli Ombay and Bartholomayo Mathias for running the Epilepsy Clinic. Our specials thanks go to the patients who were always willing to comply with our lengthy protocols. Andrea Sylvia Winkler was supported by The Centre for International Migration, Frankfurt, Germany.