
Abstract
Rapid diagnosis of tuberculous meningitis (TBM) is crucial as the disease outcome depends on the stage at which the treatment is initiated. The reliability of the available tests has not been established; thus, the present study was conducted to evaluate the conventional diagnostic tests as compared to the newer methods. Cerebrospinal fluid was collected from 100 children, and analyzed for various biochemical and cytological tests. The samples were subjected to Ziehl-Neelsen (Z-N) staining, Lowenstein-Jensen (L-J) culture, BACTEC culture and polymerase chain reaction (PCR). Twenty-two patients could be identified as definitive TBM based on the demonstration of Mycobacterium tuberculosis by BACTEC culture and PCR. Of these 22 cases, Z-N staining was positive in only two and L-J culture in six cases. Both the BACTEC culture and PCR had 100% agreement in the diagnosis of TBM. However, BACTEC culture could be a better diagnostic test as drug sensitivity can also be performed by this method.
Introduction
Tuberculous meningitis (TBM) is the most severe manifestation of extrapulmonary tuberculosis. The incidence of TBM in developing countries is approximately 7–12% of all cases of tuberculosis. 1 Rapid detection of the causative organism is important in cases of TBM, as the clinical outcome depends heavily on the stage at which treatment is initiated.1,2
Demonstration of Mycobacterium tuberculosis from cerebrospinal fluid (CSF) by direct microscopy staining or culture still remains the gold standard.1,3 However, because of their low diagnostic yield, diagnosis of TBM remains difficult.2–4
The role of BACTEC culture and polymerase chain reaction (PCR) in diagnosis of TBM have been investigated as a preliminary study,5–7 but their precise role remains undefined. Thus, the present study planned to evaluate the diagnostic value of different diagnostic tests.
Materials and methods
The study included 100 children between 6 months to 12 years of age who were presumptively diagnosed with TBM by a set of predetermined criteria.
The patients who showed presence of tubercle bacilli by Ziehl-Neelsen (Z-N) staining, Lowenstein-Jensen (L-J) culture, BACTEC culture or PCR were labeled as definitive TBM and others as probable cases.
CSF sample was collected and aliquoted for various investigations such as glucose and protein levels and for cytological evaluation. CSF smear was stained with Z-N stain and examined under a microscope (×100). It was also inoculated on L-J culture and BACTEC 12 B vial medium for the growth of M. tuberculosis. 4
Mycobacterial DNA was extracted from CSF samples as per the standard protocol.
8
Amplification was carried out using primers from Generay Biotech (Shanghai) targeting the 240 base-pair sequence of the MPB64 gene. M. tuberculosis H37Rv was used as a positive control. The amplified products were detected on 2% Nusieve agarose gel stained with ethidium bromide (Figure 1).
Gel electrophoresis of CSF samples along with positive and negative controls
Statistical analysis
All the data were analyzed using SPSS software Windows version 12.0.
Results
Of a total of 100 patients, 22 had definitive TBM as evidenced by the demonstration of M. tuberculosis in their CSF by Z-N smear, TB culture and/or PCR. The other 78 patients were labeled as probable TBM. The mean age of the study group was 4 ± 1.2 years with male:female ratio being 12:13. Most of the patients presented with fever, but other common complaints were headache and neck stiffness. There was no statistically significant difference in the demographic profile or the clinical presentation of either definitive or probable TBM groups (P > 0.05, Chi Square test).
The mean CSF protein level was significantly higher in the definitive TBM group (P < 0.001). CSF glucose levels were significantly lower in the definitive TBM group (P < 0.01).
Acid fast bacilli (AFB) on Z-N staining could be detected in only two patients, whereas L-J culture could detect it in an additional four cases, i.e. a total of six cases.
BACTEC culture and PCR results increased the yield by another 16% compared to the conventional L-J culture (Table 1). PCR was positive in 22 samples that were also positive on BACTEC culture. They were significantly correlated (Pearson's coefficient N = 1).
Comparison of results of L-J culture, BACTEC culture and PCR
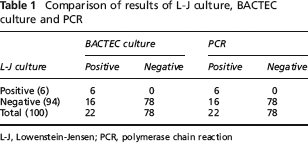
L-J, Lowenstein-Jensen; PCR, polymerase chain reaction
Discussion
This present study evaluated the diagnostic utility of different methods for detection of M. tuberculosis from CSF samples. CSF cytology and biochemical analysis could help in the presumptive diagnosis.
Z-N smear and L-J culture, conventionally considered as the gold standard, proved to be highly insensitive methods, detecting only 6% of all suspected cases. A few possible explanations offered for the lower diagnostic yield of Z-N smear and culture in our study group could be due to the high prevalence of paucibacillary disease in the study group as a result of impaired immunity secondary to poor nutrition, intercurrent infection, presence of co-morbid conditions, high prevalence of HIV disease or due to genetic factors such as NRAMP1 gene polymorphism. 4 BACTEC culture and PCR positivity of 22% is distinctly better than L-J culture for diagnosis as has been reported previously.9,10
In the present study, cytological and biochemical analysis of the CSF sample proved to be a better distinguishing factor than the clinical presentation. As BACTEC culture is equally sensitive to PCR for diagnosing TBM, we feel that BACTEC culture can prove to be a better diagnostic test, as drug sensitivity can also be performed on all the positive samples, which will help the clinicians in better management of these patients.