
Abstract
A longitudinal recruitment of adult tetanus patients to determine the survival rate of adult tetanus patients was conducted at the Lagos State University Teaching Hospital, Ikeja, Lagos, Nigeria. One hundred and sixty-four patients were admitted and forty-nine (30%) survived. The only significant determinant of survival was young age (P = 0.017).
Introduction
Tetanus is a severe disease caused by Clostridium tetani, an obligate, anaerobic Gram-positive spore-bearing bacillus. Tetanus is a medical emergency. Globally, it causes about one million deaths annually with an average mortality of 50% 1 . It is a major cause of death in children and adults in resource-poor countries located in warm humid climates. In several African countries the survival rates remain low1–6 and the social and economic burden is high. 2 The medical care is expensive and skill-intensive, and the mortality rate is high even where advanced medical facilities exist.
We report on adult tetanus cases seen at the Lagos State University Teaching Hospital (LASUTH), Ikeja. The objective of the study was to estimate the survival rate of adult tetanus and the determinants of the risk of dying from the infection within the limited resources available to our hospital.
Materials and methods
Study design
The study design was a longitudinal recruitment of all adult tetanus cases admitted through the adult medical emergency services at LASUTH between January 2004 and March 2006. This period was selected in part because the hospital was about to implement a new protocol for the management of tetanus and to establishing a dedicated, well-equipped tetanus management facility in April 2006. The clinical staff included skilled nurses and doctors but the available infrastructure and material resources were considered less than adequate. All patients were monitored by one of the authors from admission to discharge.
Data collection
Relevant information obtained from patients, or their relatives, included age, gender, date of admission, occupation and portal of entry. The information was then analysed using EpiInfo V 6.04c. Both descriptive and inferential statistics were computed in order to identify determinants of survival from tetanus. The level of significance was set at P < 0.05.
Limitations of the study
The majority of the patients were unable to communicate on admission due to trismus and spasms, and were living alone and had been brought by neighbours. Hence, important information, such as the incubation period, the time of exposure/injury, the time of onset, the severity of the disease, details of occupation and socioeconomic status, were not available for the majority of the patients. These would have been useful in identifying the role played in survival from tetanus.
Results
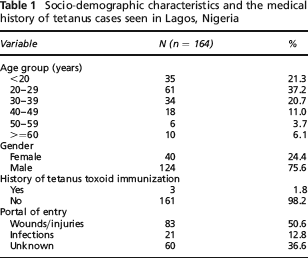
One hundred and sixty-four patients were admitted suffering from tetanus during the study period. All but two had generalized tetanus. Table 1 contains data on the socio-demographic and medical history of the patients. The mean age was 29.61 ± 12.88 years. The portal of entry was from wounds in 83 (50.6%) but unknown in 60 (36.6%).
Socio-demographic characteristics and the medical history of tetanus cases seen in Lagos, Nigeria
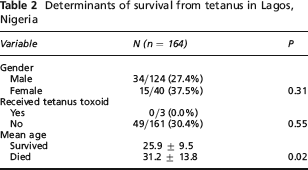
Forty-nine patients survived, giving a survival rate of 29.9%. There were 115 deaths (case fatality rate of 70.1%). The age-adjusted survival rate in the various age groups was: 37% in those under 20 years; 34% (20–29 years); 27% (30–39 years); 28% (40–49 years); 6% (50–59 years); and 0% in those above 60 years. The trend was significant (P = 0.02). Seventy-two (62.6%) of the deaths occurred within 24 hours of admission. Most deaths occurred within the first two days with a higher survival rate after the second day – there were no more deaths after the seventh day of admission. The major causes of death were severe uncontrollable spasms (41%) and cardiac arrest from autonomic dysfunction (20%). Other causes of death included: asphyxia from laryngeal spasm (10%); hyperpyrexia (10%); sepsis (8%); acute renal failure (5%); and ‘unknown’ (6%). Determinants of survival from tetanus are shown in Table 2. The only significant determinant of survival was younger age (P = 0.017).
Determinants of survival from tetanus in Lagos, Nigeria
Discussion
The peak age incidence and male dominance of the cases in this study conform with the pattern reported from Ghana. 3 This is partly related to the increased exposure to potential sources of injury and contamination of such wounds among young males. The survival rate for this study is very low, lower than previous reports from Nigeria (74%, 56%),2,5,6 Ghana (50%)1,3 and Ethiopia (73%). 4 This may be due to the large proportion of unimmunized patients, the severity of infection and late presentation: 99% suffered from generalized tetanus and 40% of the deaths occurred within a few hours of arrival in hospital, and 62.6% died within the first 24 hours after admission. The severity of the disease is a well known poor prognosticator.3,5
Other contributory factors include inadequate wound management at the health facilities, 7 poor perception of the risk of tetanus in the community and the quality of care (there was no functional intensive care unit at the hospital during the period under review).
Tetanus patients were managed in an open general emergency ward along with 20 other patients with diverse illnesses. We believe that some of the 40% deaths due to severe uncontrollable spasms might have been prevented with a neuromuscular blockade if an intensive care unit had been available. 8 However, this is an expensive option and may not be sustainable in a resource-poor country such as Nigeria. Age was the only significant determinant of death from tetanus – more of the older patients died which is in agreement with other published reports.7,9,10
This study throws up a number of challenges for tetanus care in hospitals and within the community. There is the need for a dedicated tetanus treatment area within emergency units which can provide the quality of care required by this disease. All patients with wounds and infections that could potentially lead to tetanus should receive tetanus immunoglobulin and tetanus toxoid in addition to proper wound care.
Conclusion
Thirty percent of the tetanus patients at our hospital survived. Survival rate can be increased by improved hospital care, but adult immunization and ten yearly booster doses for the immunized is considered the most cost-effective measure for survival from tetanus.
Footnotes
Acknowledgments
We are grateful for the help with the data collection given by Dr (Mrs) G Kalu, Dr (Miss) Dupe Olasemo, Dr Fagbemi, Dr Bamishile and Dr Okikiade, who were interns in the Dermatology Unit of the Department of Medicine at LASUTH during the study period. We also thank the nursing staff of the adult medical emergency department of LASUTH.