
Abstract
Patients with moderate to severe osteoarthritis of the knee underwent primary elective knee arthroplasty in a well-equipped hospital in Accra, Ghana. Our main outcome measures was the new modified Oxford Knee scores (preoperative and postoperative scores). Median preoperative and postoperative knee scores were 10 and 42.5, respectively, at last follow-up with a P value <0.05 showing the reliability and significance of the scores. The average duration of inpatient hospital stay was 10 days. Of the seven patients who had surgery, one patient developed a chest infection postoperatively and another had failure of bone graft and required a revision. There was no postoperative wound infection or joint instability. The clinical outcome for this series of patients among other factors has been good within the prevailing circumstances and this shows that knee arthroplasty in developing Africa is a reality in the horizon.
Introduction
Two-thirds of the world's population live in the developing countries. The majority of African countries fall within this category. These countries suffer from lack of access to good primary health care. In 2001, injuries accounted for approximately 5.1 million deaths (about 20% of which are preventable with simple surgical intervention) and for approximately 12% of the disability-adjusted life years lost worldwide – more than those lost as a result of TB (2.5%), diarrhoea (4.3%), malaria (2.9%), human immunodeficiency virus (HIV, 6%) or cancer (5.2%). Although, worldwide, injuries are the main cause of death among those aged between 5 and 40 years 1 less attention is paid to them than other important diseases such as communicable diseases, malaria, HIV/AIDS and nutrition. In sub-Saharan Africa few can afford western style treatments for chronic orthopaedic trauma-related conditions. However, trauma is becoming a major cause of morbidity and mortality in African countries such as Ghana. 1–3 Perhaps re-directing funds from those who could afford to pay for the more expensive treatment to the establishment of low cost but effective orthopaedic trauma care for all could be a strategy which, at the same time, might help to improve the local healthcare resources.
Charities and voluntary health organisations have attempted to alleviate the problems associated with orthopaedic-trauma/health care in the developing world. However, most have based their projects on foreign sponsored projects that are dependent on the enthusiasm of the organisations and the funds available. 4 In addition, most have been reluctant to introduce any projects that will cost the foreign sponsor too much money. As a result, there has been considerable difficulty in trying to improve local services and to provide high technology orthopaedic trauma services. There are a few exceptions, for example the scheme by Professor John Jellis in Zambia which provides free clinical services to paediatric patients with musculo-skeletal deformities from income generated from treatment paid for by the more affluent patients. 5
Motec Life – UK is a multi-disciplinary charity based in the UK whose aim is to develop self-sustaining orthopaedic trauma care providing low cost but effective treatment for targeted populations in developing countries such as Ghana. Multi-disciplinary teams provide education and transfer of skills to the local health workforce which reciprocates by relating their experience to the Western-based health worker in clinical scenarios in developing countries and also for those dealing with medical conditions afflicting minority ethnic populations in the western world. 6,7
In 2005, the number of recorded primary total knee joint replacements in England and Wales was over 59,000 8 and many papers have been published on knee arthroplasties performed in the developed world. However, there is very little published literature on the outcome of knee arthroplasty in Africa, although such operations are being carried out in South Africa, Malawi, Zambia and some Northern African countries. 5,9
Motec's reports on current practices in Ghana show that conservative treatment for osteoarthritis would be the first choice for most, with fusion of the knee with unlocked intra-medullary nail being the most affordable surgical option in areas where support for rehabilitation is non-existent. We could not imagine the kind of life a patient would enjoy with bilateral fused knees anywhere in the world, let alone sub-Saharan Africa where there is lack of support services for mobility, home adjustments and activities of daily living. Although high tibial osteotomies or double osteotomies of the knee involve very low surgical costs, those working in local health centres throughout the developing world do not always have the skills required to perform such operations and to rehabilitate patients. In addition, the prolonged rehabilitation period after osteotomies poses a bigger challenge as there is a relatively low life expectancy and many young patients are the main breadwinners. Appropriate implants such as those developed for the Asian market which provide early mobility and return to work could be of great use in the developing countries.
In this article, we report on a series of seven patients who underwent eight primary knee arthroplasties in a private setting in Accra, Ghana. The overall objective is to give an idea of knee joint arthroplasty in developing Africa.
Patients and methods
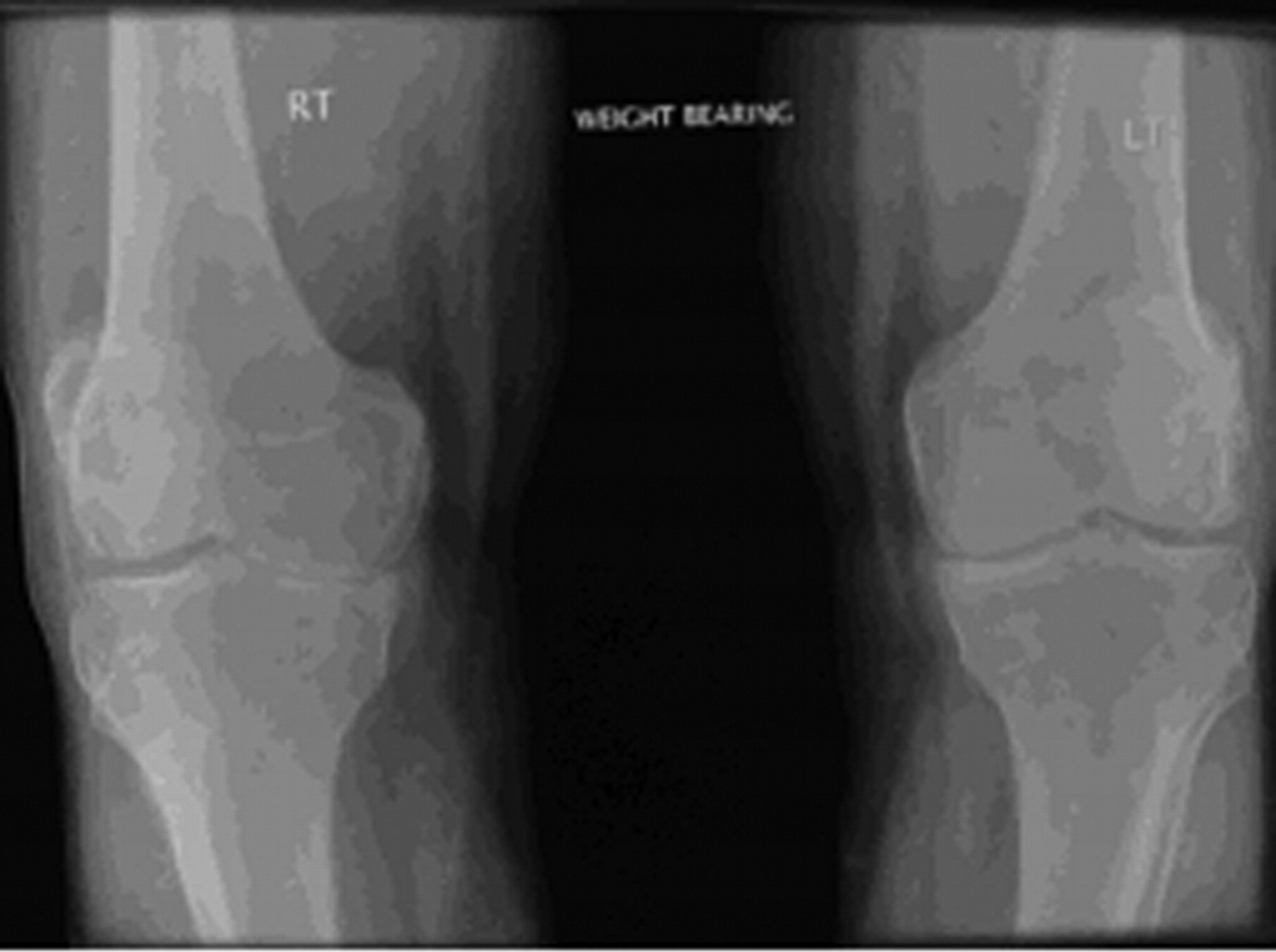
Data on patient demographics were collected prospectively. A series of patients underwent primary knee replacement between October 2006 and October 2007 (Figures 1 and 2).

Patient 1: posttraumatic bilateral knee osteoarthritis with multi-ligament insufficiency. (a) Right knee; (b) left knee
Patient 2: bilateral knee osteoarthritis
The patients in this series were those who could afford to pay about £3500 for the procedure. Knee arthroplasty surgery was performed in a well-equipped private hospital in Accra with Motec providing the surgical and peri-operative rehabilitation team. Seven of the procedures were undertaken under spinal anaesthesia, and one under general plus sciatic and femoral nerve blocks. The procedures were carried out by one of the authors (P Ofori-Atta). Routine doses of intravenous cephalosporin (Zinacef, GlaxoSmithKline) at induction and two further doses post-operatively, were given as prophylaxis. A tourniquet was used in all but one patient with sickle-cell haemoglobinopathy. Deep vein thrombosis prophylaxis included a combination of self exercises (ankle and foot), low-molecular weight heparin and aspirin. The indications for surgery were severe symptoms of advanced knee osteoarthritis and failed conservative treatment (Figures 3–7).
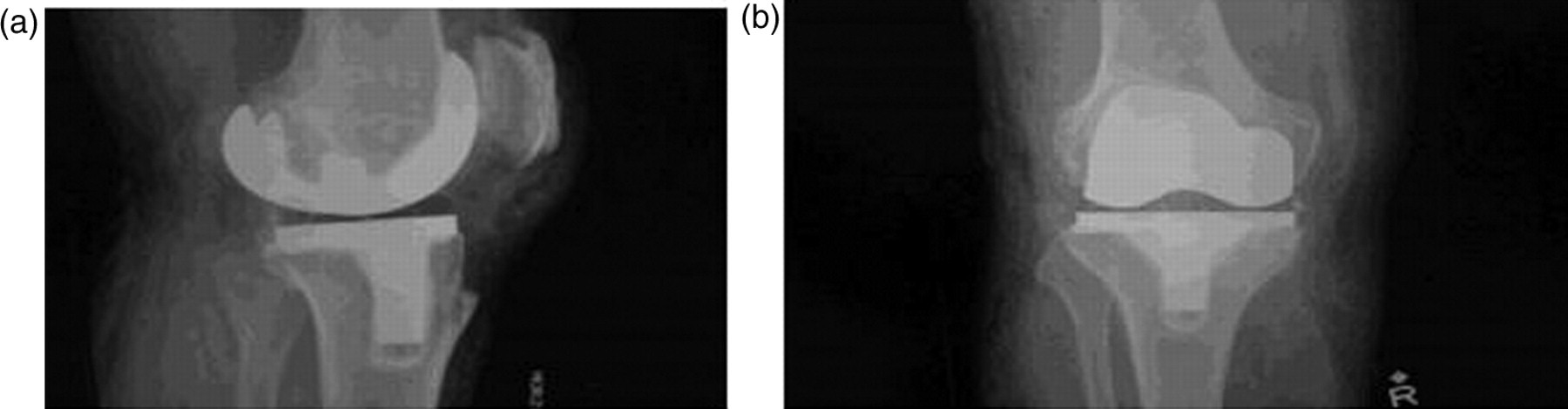
Patient 3: post right total knee replacement X-rays

Patient 4: four days postoperatively
Patient 5: three months postoperatively. Patient with 45-year-old knee replacement with post-traumatic osteoarthritis, multi-ligament insufficiency. The right knee was more badly affected

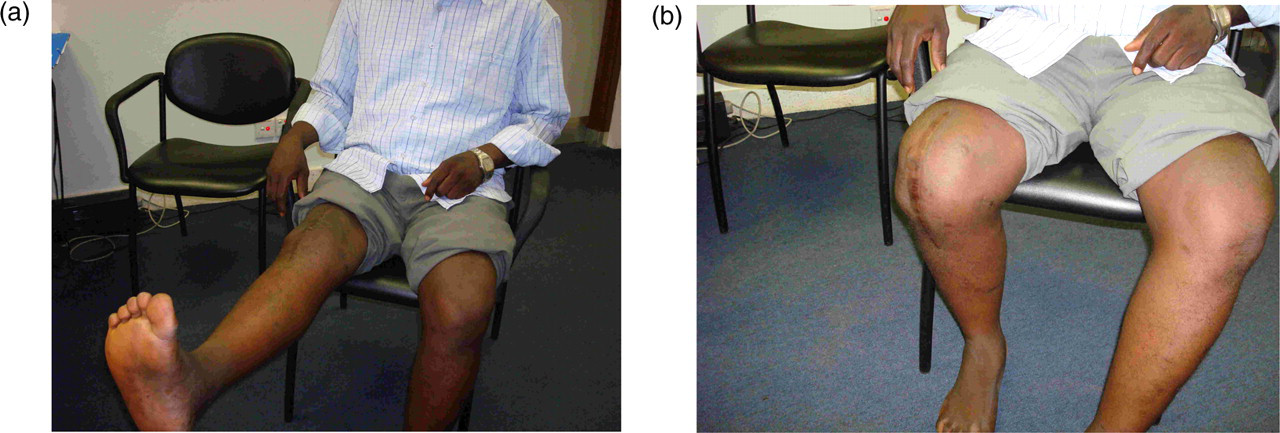
Patient 6: mobilization. (a) Early post knee replacement; (b) at six months after replacement

Patient 7: four months after revision of total left knee implant for failed bone graft
Questionnaire
The new Oxford Knee Score questionnaire 10 was used as the primary outcome measure of success. This is a functional score that helps to assess the impact of knee pain on daily activities and which indicates a higher score for better function and less for knees with pain and disabling symptoms. For practical purposes the patient questionnaires were completed by telephone. The data were collected by one of the authors (A O George).
Follow-up
Patients were assessed clinically and post-operatively in the follow-up clinic. This was done by the primary surgeon, and features such as range of movements, signs of infection, knee stability, level of pain and level of function were assessed. Patients were examined, and their hospital records also checked (A O George) in Accra. There were neither clinical deep vein thromboses nor pulmonary embolisms.
Statistics
All data collected was stored and analysed on Microsoft Office Excel (2003 version). The data collected was found to be nonparametric. The Wilcoxon's text was used to compare paired continuous data and the chi-square test was used to analyse categorical data. A P value of less than 0.05 was deemed significant (Tables 1 and 2).
Pre- and post-operative responses from patients using the Oxford Knee Scores questionnaire
Pre- and postoperative Oxford Knee Scores
Patients
There were a total of seven patients (six women and one man) who underwent eight knee replacements. Six had press fit condylar rotating platforms and two had posterior stabilized semi-constrained arthrogryposis multiplex congenita knees. The age range was between 38 to 71 years with an interquartile range (IQR) of 24 and a median quartile age of 59.3 years. The youngest patient (aged 38) had posttraumatic knee osteoarthritis: four had an American Society of Anaesthetist grade of 1, one had grade 2 and two grade 3. The follow-up period ranged from three months to one year with a mean of six months.
Surgery
The average duration of in-patient hospital stay was 10 days with a range of five to 12 days. Six patients had an uneventful postoperative recovery; one patient had a chest infection on the third day after surgery; and another had failure of bone graft of a large tibial plateau defect that required revision of the tibial implant.
Functional score
Median preoperative knee scores were 15.5 (IQR 5.0 – 26.0). Median postoperative Oxford Knee Score was 44.5 (IQR 32.5 – 51.3). There were significant differences between pre- and postoperative scores for this group of patients (P value ≤ 0.007812).
Follow-up
At a median follow-up of six months, there was no postoperative wound infection and no joint instability. The first postoperative review was between six and 12 weeks and second review at about six months to one year.
Discussion
The P value (<0.05) in this data shows the significance and reliability of the data.
This study is limited by a small sample size and a short follow-up, but it provides an opportunity to shop for total knee replacement solutions for sub-Saharan African. Studies are ongoing in order to review the long-term outcome of a larger patient study but, at this stage, the audit provides a snapshot of the evolving experience in this setting.
There were only eight operations on seven patients. Therefore the sample size may not represent the normal demography in the general population. In addition, the surgical team only paid short visits and provided a limited service to only a few. Patient selection was based on symptomatic advanced osteoarthritis that had failed with conservative management, and also on the patient's ability to afford the surgical management.
The average cost of a knee replacement, including hospital stay/care, is about £3500 – about a third of the cost of a private operation in England. Money generated from this service was put directly into the management of debilitating orthopaedic trauma conditions (such as non-union of long bones) and the provision of educational workshops in Motec's target hospitals in Ghana. Also, funds generated were used to provide equipment such as tourniquets, patient monitors for the recovery wards and image intensifiers for the rural based target hospitals. In spite of the reduced cost, many ordinary Ghanaians would be unable to afford the service. However, the demand from wealthier patients is high with a waiting list of over 50 people. One patient with delayed presentation who had failed with arthroplasty following bone graft failure would have done well with an appropriate metal wedge in the first instance. Biological efforts must certainly be considered in Africa if alternative and effective biological methods are to supplement artificial treatments.
The average duration of postoperative inpatient care was high compared with western standards, but there are a number of reasons for this. Physiotherapy has been shown to shorten hospital stay 11 and in Ghana there is limited physiotherapy expertise for post-operative services. Motec had to resort to in-service training of a local physiotherapist whose post discharge services were paid for separately by patients. There are no rehabilitation centres other than hospitals for patents. Social back up arrangements seemed to be reasonably satisfactory for the patients who could afford the service. There are serious doubts about poorer patients who might have to rely on the very limited public services for basic hygiene and life activities at home. In the large African family context this may not always be seen to be a problem.
From our results, knee arthroplasty in Africa seems feasible. There is overwhelming evidence that osteoarthritis of the knee has a great effect on the lives of people in low and moderate income economies such as sub-Saharan Africa. 1 The availability of high quality health care can influence the overall economic activity of a nation. For example, a heavy disease burden leads to decreased per capita production, which in turn causes decreased economic development. 1,4 It is difficult for poor nations to include the cost of expensive surgery in their budgets. On the other hand, if those who can afford discounted high technology surgery paid indirectly for some of the less high technology orthopaedic treatment, the burden on the budgets could be reduced significantly. Education could play a vital part in a strategy to improve orthopaedic trauma care in Africa. 7
Limited though epidemiological data is on the burden of musculo-skeletal diseases in sub-Saharan Africa, the indications are that orthopaedic trauma conditions are on the increase in countries like Ghana. 2 The implications are that improvements in health care could generate improvements in basic health care for the majority of the population.
Working visits by health-care experts to a developing country which is immersed in a health-care culture and system totally different from the developed world brings a unique set of opportunities and rewards. There would be a two-way exchange of ideas and education, a transfer of skills between health-care workers, an opportunity to discover effective ways of developing local methods to improve and develop sustainable local services and projects with a little help from abroad. The focus should be on helping sub-Saharan economies find the ways and means to address their local resource shortfalls – human, capital and service – rather than to condemn advancement in Africa based on the over-emphasis of the communicable disease burden and services that have to rely on short-lived handouts. Appropriate implant surgery for those who can afford it in low to moderate income economies should be encouraged in order to provide basic but effective treatment for musculo-skeletal conditions.
In Malawi, at the Beit Cure International Hospital is a model worthy of emulation. The centre, in the main, is a children's orthopaedic hospital that receives its funding from charities, the main ones being The Beit Trust UK and Cure International. It provides 50 beds for children and has a private adult orthopaedic wing. Any funds generated by the private work go to support the free operations. Last year 13% of all surgery carried out in the hospital were privately funded, and the target for 2008 will be 25% in order to sustain the provision of a free service for children and the poor. The private patients love this model and feel very involved with the children as a result. Many go on to make donations. 12,13
Motec Life UK does not have its own hospital but it is hoped that as a result of the experiences acquired in the experimental phase of voluntary work in Ghana, coupled with the working model in Malawi, some form of an organizational structure utilizing the existing facilities could be modelled to help patients in Ghana.
From the results in the series, there are a lot of indicators for hope for knee arthroplasty in developing Africa. The principal findings of this study are:
Total knee arthrolasty can be undertaken in an African setting; It is safe (although there was one revision for a failed bone graft and one recorded postoperative chest infection); The results are beneficial and probably cost effective as there was a significant improvement in the Oxford Knee Score postoperatively (see Table 1).
Footnotes
Acknowledgements
Both authors are members of the UK registered medical charity Motec Life UK.
We are grateful to Professor Chris Lavy and Mr Jim Harrison, who are both trauma and orthopaedic surgeons at the Beit Cure International Hospital in Malawi, for their invaluable help with the preparation of this paper.