
Abstract
This study was undertaken in order to evaluate the feasibility and safety of performing laparoscopic orchidectomy (LO) in men for unilateral impalpable testis in non-teaching rural hospitals in a developing country. We also investigated the possibility of reducing the cost and length of stay in hospital for patients undergoing LO. This is a prospective analysis of patients with impalpable testis undergoing LO in three non-teaching rural hospitals in the Kashmir Valley from January 2001 to March 2007. The cohort represented men requiring LO aged 15 to 62 (mean 36.2) years. The main outcome parameters assessed included mortality, conversion to an open procedure, complications, reduction in the costs and the length of the hospital stay.
Forty-eight men with unilateral undescended testis on physical examination were studied. During laparoscopy the testis was identified near the deep ring in 30 patients, intra-abdominally in 16, and two had blind-ending vas and spermatic vessels near the deep ring. In 46 patients orchidectomy was performed. There were no deaths and none of the patients required conversion to an open procedure. Using reusable instruments, 00° polyglactin sutures and self-made extraction bags, about US$ 300/patient was saved. There was no case of malignancy of the testis on histopathology examination. LO is one of the most satisfactory methods for the management of men with impalpable testis, having both a diagnostic and a therapeutic role especially for patients in the underdeveloped countries. These simple methods can reduce the cost and the length of the hospital stay.
Introduction
The occurrence of torsion, trauma, tumours and reduced fertility and complications in patients with maldescended testis have been well documented.1–3 The ideal treatment for such patients is orchidopexym preferably by the second year of life. To prevent damage to the sperm-forming cells it is important to place the testis in the scrotum where the temperature is lower temperature than in the abdominal cavity. 4
Unfortunately, in the developing countries some patients do not present until adulthood. By that time the damage to spermatogonia has already occurred and hence the treatment options change.1,2 Some authors recommend orchidopexy with regular follow-ups as the treatment of choice even in adults. 5 This is done with a view to utilizing the hormone production of the testis and a few have reported spermatogenesis in undescended testis. 5 However, the increased incidence of malignant transformation in undescended testis, even if placed in the inguinal canal or the scrotum, remains the main indication for orchidectomy in such cases. 6
If the testis cannot be palpated during physical examination, high resolution ultrasound (HRUSG) should be the first investigative modality used to note the location and the physical characteristics of the gonad7,8 but magnetic resonance imaging (MRI) can also be used.9,10 However, the pick-up rate for these investigations is only 68%–91%.7,11
Until recently the testis would be removed by an open method such as an exploratory laparotomy.12,13 The success of laparoscopic cholecystectomy led surgeons to explore other areas for its use such as in the management of undescended testis. Laparoscopy is a one step diagnostic and therapeutic tool. 14 The magnified view of the vas deferens and the testis in the abdominal cavity, and the ability to perform the required surgical intervention in the same sitting, allows the laparoscopic method to score over other diagnostic modalities and the open surgery.14–18
In developing countries such as India, laprocsopic orchidectomy (LO) has greatly reduced the financial burden for patients where the daily income is around US$ 2 a day. 19 The early recovery allows the patient to return to work quickly which is a great advantage if he is the only breadwinner.
This clinical study was conducted in order to examine the feasibility and safety of performing LOs in small hospitals in a developing country and to reduce the overall hospital stay and the costs associated with LO.
Patients and methods
The study was conducted in different hospitals in the Kashmir Valley from January 2001 to March 2007. Adults undergoing diagnostic laparoscopy and LO for impalpable testis were the basis of this study. Only patients over 14 years of age were included. Patients with cardiovascular instability or coagulation abnormalities were excluded. Those with a palpable testis in the inguinal canal, or a presence of testis-like structures in the inguinal canal suggested by HRUSG, were also excluded.
The selection of which patients should undergo laparoscopy or LO was made on the basis of their history and physical examination. HRUSG was used as the initial tool for locating the testis.
Informed consent was obtained after a detailed discussion with the patient and his attendants about the benefits and possible complications. The patients were informed of the long-term results and complications of undescended testis, orchidopexy and orchidectomy. In order to reduce the length of the hospital stay, patients were allowed to have liquids up to six hours before the operation and were admitted on the day of surgery.
Operative details
For diagnostic laparoscopy, a 5-mm 30° telescope was introduced at the umbilicus. Two working ports, one 5 mm located in the iliac fossa on the side of the undescended testis and a 10-mm supra pubic port, were used for patients selected for orchidectomy. After the initial laparoscopy the procedures were as follows:
Group A If a blind-ending vas and spermatic vessels were detected terminating near the deep ring, no further treatment was instituted.
Group B If the testis was located near the internal ring without any associated hernia, we dissected the covering tissues the testicular artery and the vas deferens were separately clipped or ligated with polyglactin sutures. After excision of the testis, the specimen was removed in a self-made endobag made from the inner sterile cover of the Ryle's tube of a 10-mm supra pubic port.
Group C If the testis was located free in the abdominal cavity, the procedure for group B was followed after the testis was lifted clear of the surrounding structures.
In the postoperative period the patients were allowed oral liquids as soon as nausea was overcome. Early ambulation was advised. The patients were usually discharged on the first postoperative day. Follow-up was done at one week, four weeks and three months interval.
Results
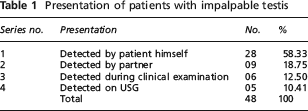
The present study was comprised of 48 patients, aged 15 -62 years (mean 36.2) with unilateral impalpable undescended testis who presented to various hospitals in the Kashmir Valley from January 2001 until March 2007. The mode of presentation is documented in Table 1.
Presentation of patients with impalpable testis
Of these 48 patients, 33 had an impalpable testis on the right side and 15 on the left side. There were no cases of bilateral cryptorchidism.
A local examination was unable to identify the testis in any patient. HRUSG was used to locate the testis, or testis-like structures, near the deep ring in 16 patients and in 14 the testis was located in the abdominal cavity.
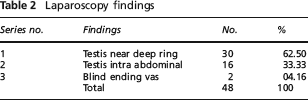
The laparoscopy findings are documented in Table 2. The average operating time was 28 min (range 8 min to 70 min). In cases where only diagnostic laparoscopy was required the average time taken was 10 min. There were no conversions to an open procedure and no intraoperative complications. Bleeding was minimal. In the postoperative period the patients were allowed oral fluids within six to eight hours. Eleven complained of right shoulder-tip pain which subsided on its own. Two had port site sepsis managed by local hygiene.
Laparoscopy findings
The length of hospital stay range was 8–29 hours (mean 21 hours). Two patients had to stay in the hospital for more than 24 hours for various reasons. The majority were back to work within one week of surgery.
There were no deaths in the immediate 30-day period and we did not come across any complications related to the procedure.
Discussion
Even though laparoscopic orchidopexy is considered to be the treatment of choice for children,15,17,19 there are very few published reports on the management of adults with undescended testis and they are conflicting.5,15,19 In the developed world it is rare to see a patient of undescended testis presenting in adulthood, but the situation is quite different in the developing countries where patients over the age of 30 have presented. 19 The reasons for this are multifactorial. Overall low literacy rates, and specifically the lack of sex education, among the general population and poor access to health-care facilities are the main reasons for such late presentation. 19
The overall accuracy of radiologic testing for the undescended testis is 44%–91%.7,11,20 As surgical exploration is eventually necessary, imaging is a fruitless and expensive endeavor that, in most situations, does not influence the decision to operate, the surgical approach or the viability or salvageability of the cryptorchid testis. Many modalities have been employed including ultrasound,7,20 computerized axial tomography scanning, 7 MRI,9,10 testicular angiography 7 and venography, pneumoperitoneography and herniography. Many are either invasive, require anaesthesia, are technically difficult to perform or are associated with a significant rate of false-negative results.15,21,22 In developing countries, the availability and the cost factor of these investigations has to be taken into consideration. Hence, our approach was to subject the patient first to a high resolution ultrasonography 7 followed by a diagnostic and therapeutic laparoscopy.
The incidence of testicular tumours in the general population is one in 100,000, and the incidence of a germ cell tumour in men (cryptorchid) is one in 2550. Therefore the relative risk is approximately 40 times greater. 23 The risk of malignancy does not decrease even if the testis is placed in the scrotum. In addition, repeated physical and radiological follow-ups of such patients are required in order to monitor the development of malignancy. 24 In our series patients chose orchidectomy as their treatment option. The relative size of the testis had no bearing to the surgical intervention after counselling. Patients with undescended testis usually belonged to the poor socio economic class and were usually from rural areas. As repeated follow-ups 25 were uneconomical, they requested an orchidectomy rather than an orchidopexy. We did not find any cases of testicular malignancy or any other abnormality in the specimens during the histopathology examinations 2 ; however, one study from India reported that almost 14% of testicular tumours were found to be in the cryptorchid testis. 26
There were no deaths or major morbidity in our series.6,27 The mean operating time was 28 min (range 8–70 min). If only a diagnostic laparoscopy was required the procedure took approximately 10 min. Eleven patients complained of post surgery shoulder-tip pain. Only two complained of port site sepsis. The specimens of the testes removed showed uniform atrophy of the seminiferous tubules. 15
Laparoscopy stands alone as having both a diagnostic and a therapeutic role. The exact location of the testis can be identified by following the vas on the corresponding side. If the vas terminates blindly it is diagnosed as a case of vanishing testis syndrome.4,16 Otherwise, on identification of the testis, orchidectomy or even orchidopexy can be performed by laparoscopic method alone.14–18 The benefits of the minimal access technique are more relevant in the underdeveloped world. The minimal pain, early discharge from the hospital and quick return to work are of considerable financial benefit to the patients. To minimize the costs associated with the procedure 00° polyglactin sutures can be used instead of expensive ligaclips. The specimen can be extracted in a self-made endobag made from the inner sterile cover of a Ryle's tube as reported in an earlier report of a gall bladder extraction. 28 We used reusable sterilized hand instruments and trocar cannulae without any increased complication rates. By these simple means we managed to save around US$ 300 per case which is equivalent to 150 days pay in our region.
Conclusion
Adults with undescended impalpable testis are still found in developing countries. On counseling, these patient usually choose orchidectomy as the preferred treatment procedure. The proven benefits of the laparoscopic method can also be extended to these patients. LO can be performed safely even in the nonteaching hospitals in the developing countries. Around US$ 300 can be saved for each case of LO if the simple measures documented above are taken. The introduction of sex education in schools could help to reduce the late presentation of patients with undescended testis.