
Abstract
We present a case series of patients who underwent simple perianal procedures outside this hospital but developed postoperative and life-threatening retroperitoneal necrotizing fasciitis. With a high index of clinical suspicion and radiological imaging, we were able to establish earlier diagnosis. Resuscitation, the use of intravenous broad-spectrum antibiotics, aggressive surgical debridement and continuous organ support were essential in achieving a positive outcome in both of these patients.
Introduction
Necrotizing fasciitis (NF) is an acute surgical condition which demands prompt recognition, resuscitation, broad-spectrum antibiotic therapy and aggressive surgical debridement. Retroperitoneal NF is a rare but potentially fatal complication of perianal procedures. The lack of external clinical signs results in delayed diagnosis and the local anatomical barrier makes aggressive debridement extremely difficult. The authors present two cases of retroperitoneal NF which developed after relatively minor perianal procedures.
Case history
Case one
A 42-year-old diabetic male presented as an emergency with a history of recent incision and drainage of a perianal abscess at a different hospital. On arrival he complained of a two-day history of intermittent fever, lower abdominal and incision site pain and loose watery stools. On examination he looked toxic and dehydrated and was tachycardic and tachypnoeic. His abdomen was distended with erythema and tenderness inferiorly. The perineum and scrotum were swollen with a 2 × 3 cm wound in the left lateral position. Laboratory results showed a pancytopaenia, compromised renal function and hyponatraemia. A computerized tomography scan of his abdomen showed extensive soft tissue oedema, multiple fluid pockets and free gas in the retroperitoneum (RP) (Figure 1).
A computerized tomography scan of the abdomen showing retroperitoneal necrosis with gas formation
After fluid resuscitation and the administration of broad spectrum antibiotics, the patient was taken for surgical exploration and debridement. He was placed in the lithotomy position to allow access to both RP and the perineum. The abdomen was explored via a midline incision and 2 L of pus were found in the RP, extending from pelvis to diaphragm and to the lateral abdominal wall. The perineal wound and necrotic tissue in the RP were extensively debrided and a transverse loop colostomy was fashioned. The debrided sites were washed out and multiple drains placed into the RP, pelvis and perineum. The abdomen was closed using a vicryl mesh (Figure 2). Pus and necrotic tissue submitted for culture grew polyorganisms and antibiotics were continued accordingly. Tissue sent for histology confirmed NF. The patient was kept intubated and ventilated and was taken for relook laparotomy 48 h, at which no evidence of progression of the NF was found.
After debridement of the retroperitoneum, colostomy, drain placement and abdominal closure with vicryl mesh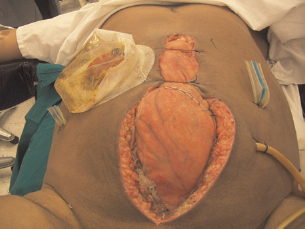
Postoperatively the patient developed acute respiratory disease syndrome and pneumonia and required ventilation on the intensive treatment unit. Nasogastric feeding was started immediately. The external wounds were dressed daily. On day 25, the infection progressed to the left thigh and further debridement in theatre was performed. On day 40, the patient developed bleeding from the colostomy, requiring resuscitation and transfusion. He remained haemodynamically unstable and mesenteric angiography revealed bleeding from the right colic artery which was successfully embolized. After 60 days in hospital the patient was discharged but attended as an outpatient for daily dressings. Subsequently, the colostomy was reversed and he is now awaiting repair of his large abdominal incisional hernia.
Case two
A 32-year-old obese male presented to the emergency room having undergone a lateral sphincterotomy for an anal fissure at another hospital. He complained of severe bilateral lumbar pain, abdominal distension, fever and vomiting since his operation. On examination he was tachypnoeic, tachycardic and hypotensive, with cold, clammy extremities. Abdominally he was distended with right-sided tenderness. There was abdominal wall, scrotal and perineal oedema and erythema with tenderness around the sphincterotomy wound, but no purulent discharge. Investigations showed a severe metabolic acidosis, a depressed white blood count of 3.2 × 109 and an elevated troponin due to a recent cardiac event. He was moved to the coronary care unit where he received fluid resuscitation, inotropic support and empirical broad-spectrum antibiotics. An abdominal computerized tomography scan showed diffuse inflammatory changes within the peritoneal cavity and focal dilatation of jejunal loops.
The patient's condition deteriorated and he was therefore taken for exploratory midline laparotomy in the lithotomy position. The main finding was retroperitoneal NF extending up to the diaphragm, with mild ascites and bowel oedema. The perineal wound was communicating with the pelvic cavity. Approximately 500 mL of pus was evacuated and the RP was debrided. Multiple open drains were placed in the pelvis and RP and the abdomen was closed using vicryl mesh. The pus submitted for culture grew polyorganisms and appropriate antibiotics were continued. At relook laparotomy 24 hours later, there was no evidence of progression of the NF. After a period on a ventilator, a postoperative pneumonia and nasogastric feeding, the patient was discharged home on day 25 for daily outpatient dressings. His abdominal wall incisional hernia has subsequently been repaired and he has resumed normal activities.
Discussion
Necrotising soft tissue infections can be classified by the type of infecting organism, the clinical presentation or the treatment required. However, reliance on any schema is impractical as it often leads to delay in appropriate surgical therapy with loss of limb or life. 1 Early radical surgical excision of all affected tissue is the treatment of choice, regardless of tissue loss. 2 A mortality rate of 37% has been reported in patients with retroperitoneal NF, in whom adequate debridement is hampered by anatomical barriers. 2 Immediate fluid resuscitation and broad-spectrum antibiotics until organism sensitivities are available are also vital elements in the management of the patient. We strongly recommend early postoperative enteral feeding to help prevent transmigration of bacteria from the gastrointestinal tract and stress ulceration. We also advocate relook laparotomy after 24–48 hours to reassess and redebride if indicated. The halt of progression of the infective process is a good prognostic sign and can be used to plan further management. The postoperative course is complicated by overwhelming sepsis resulting in multiorgan impairment. Both our patients needed ventilation and developed ventilator-associated pneumonia. Moreover, comorbidity – diabetes, obesity, cardiac disease in our cases – will further impair the outcome.
There are a few cases reported of survival after retroperitoneal NF. Paya described a 4-year-old-girl who developed this secondary to pyelonephosis 3 and Pryor reports a patient who presented with modified Grey Turner and Cullen's signs after uncomplicated haemorrhoidectomy. 4 Both were treated with aggressive debridement and antibiotics.
Above all, it is important to have a high index of suspicion of retroperitoneal NF in any patient who presents with a recent history of perianal surgery and who then develops fever and disproportionate pain but has few local clinical signs. It is easy to miss the diagnosis or underestimate the severity of the condition. The policy of prompt diagnosis, resuscitation and timely radical surgical debridement should be followed to achieve optimal outcome.