
Abstract
The present study highlights eight cases of pulmonary nocardiosis diagnosed during the time period of January 2006–March 2008. Nocardia otitidiscaviarum, N. asteroides and N. brasiliensis were isolated from these cases. Whereas six patients were treated successfully, one showed partial response and one case expired before the institution of treatment. Early and correct microbiological diagnosis can help to decrease the disease-related morbidity and mortality.
Introduction
Pulmonary nocardiosis is a subacute or chronic suppurative lung disease usually seen in immunocomprised people. It is caused by Nocardia, which is a soil-borne, opportunistic, aerobic, Gram-positive filamentous actinomycete. 1 In the USA, there are an estimated 500–1000 new cases every year. 2 In India reports are scanty and no information of the annual incidence is available, perhaps as a result of underreporting and a lack of awareness. In spite of its omnipresence in nature, the following species are known to be infectious in man: Nocardia asteroides, N. brasiliensis and occasionally N. otitidiscaviarum (formerly N. caviae). 3 The usual mode of infection is the inhalation of airborne spores or fragmented cells and is facilitated by the dry, dusty and arid climate. 4 Pulmonary infections are usually produced by N. asteroids (85%), whereas N. brasiliensis causes cutaneous and subcutaneous abscesses. 2 Patients undergoing immunosuppressive therapy, organ transplant, or with underlying causes such as tuberculosis, acquired immunodeficiency syndrome (AIDS), diabetes mellitus and alcoholism are at risk. 5 The present study evaluates the clinical features, evolution, treatment response and prognostic factors of pulmonary nocardiosis from the southern part of India.
Methods
We reviewed all consecutive cases of pulmonary nocardiosis from January 2006 to March 2008 who were seen in our tertiary care teaching hospital. Gram-staining of various samples like bronchoalveolar lavages (BAL), pleural fluid and sputum revealed numerous Gram-positive, thin beaded branching filaments that disclosed acid-fastness with modified Kinyoun acid-fast staining (Figure 1). A minimum of two samples of sputum that satisfied the Bartlett grading were taken. Growth after 48 hours on sheep blood agar, sheep chocolate agar and Sabouraud's dextrose agar incubated aerobically at 37°C was confirmed as Nocardia based on colony morphology and staining reaction. All the Nocardia isolates were later speciated using a battery of biochemical tests. 1 Antibiotic sensitivity testing was done for amikacin, imipenem, cefotaxime, trimethoprim-sulphamethoxazole (TMP-SMX) and linezolid by the disk diffusion method according to the Clinical Laboratory Standards Institute guidelines (CLSI). 6 Medical records were checked for all diagnosed cases and relevant clinical details were noted.
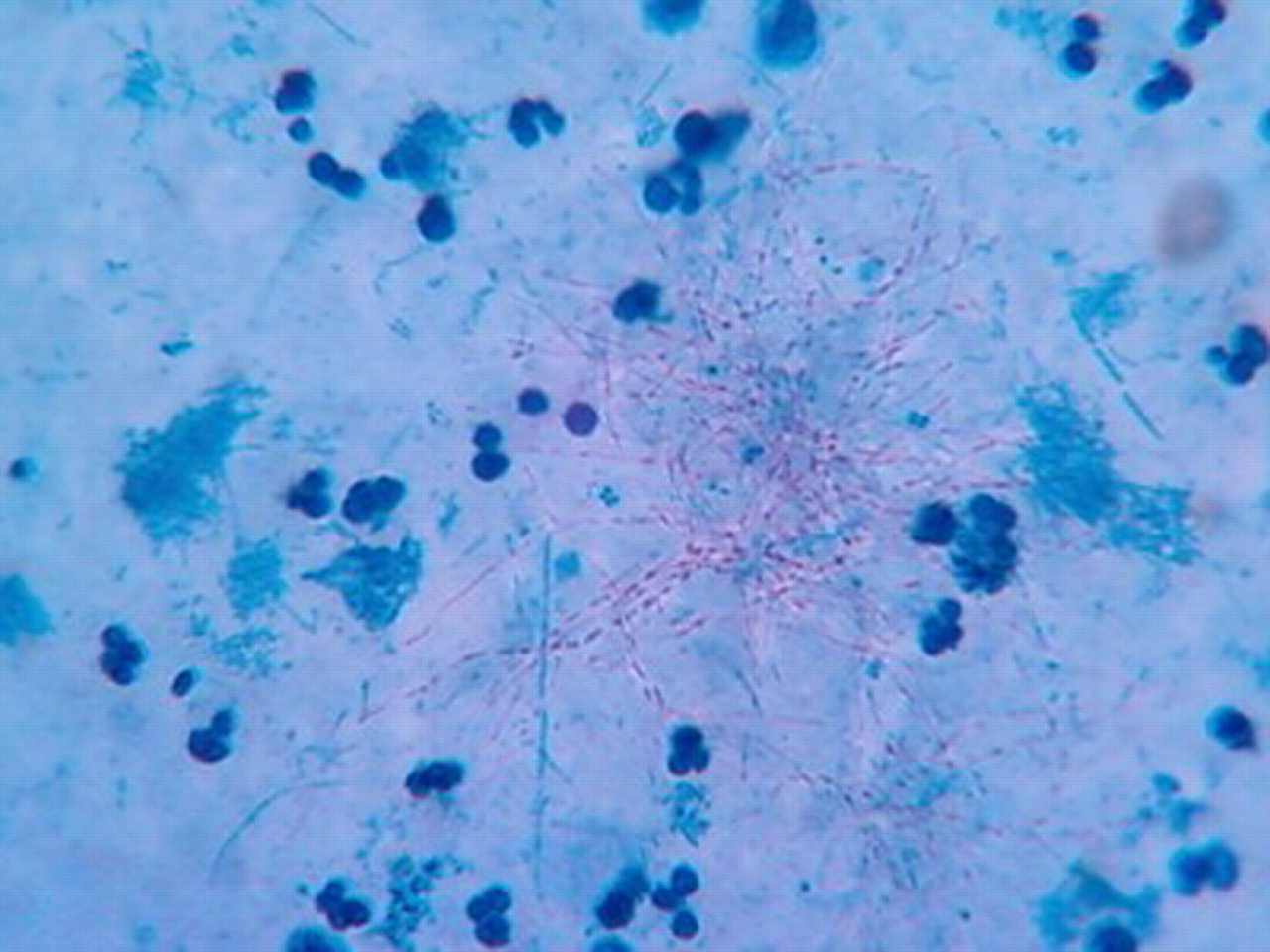
Kinyoun staining showing partially acid-fast, beaded filaments of Nocardia
Results
Eight cases were reported. The infected patients were aged 17–62 years and the male to female ratio was 3:1. The demographic, clinical and microbiological details of eight cases of pulmonary nocardiosis are shown in Table 1.
Demographic, clinical and microbiological profiles of eight cases of pulmonary nocardiosis
ATT, antitubercular therapy; BAL, bronchoalveolar lavage; TB, tuberculosis
Discussion
Pulmonary infections by Nocardia are commonly seen in immunocompromised individuals, although infection in immunocompetent persons can occasionally occur. 7 In the present series the disease was primarily observed in adults and immunocompromised persons with live related renal transplant, pulmonary tuberculosis, chronic obstructive pulmonary disease on irregular steroids and HIV, which is usual. 8 Males were more likely to be infected than females, which may be due to a greater exposure to the external environment or to some hormonal effect; 8 however, the exact cause for the gender bias is unknown.
In contrast to the usual second- to sixth-month post-transplant period when the patients have a greater propensity to opportunistic infections, 2 one patient presented two and half years and another one year after renal transplant. The post renal transplant cases were on triple immunosuppressive treatment (tacrolimus, prednisolone, azathioprine), which might well be a risk factor. The isolated strain of N. otitidiscaviarum from both the post renal transplant patients is itself a rare cause of pulmonary disease, and primarily is isolated from cutaneous or subcutaneous infections. 9
Pulmonary nocardiosis can present as an indolent or sub acute disease with symptoms being present from one to several weeks, and patients may present with cough, fever, malaise or weight loss. All our cases of pulmonary nocardiosis presented with complaint of purulent sputum: three had chest pain and breathlessness as the main complaint; four had a history of haemoptysis; and one had post-transplant weight loss of 5 kg in two months. Clinical and radiological parameters have poor predictive value in the identification of the microbiological nature of respiratory tract infections in immunosuppressed patients. 10 The varied radiological presentations, as we noticed in our study can be mimicked by many other infections, especially in immunocompromised patients. 7 The microbiological identification of the aetiological agent is therefore mandatory for the initiation of suitable treatment. Direct microscopy of Gram-stained smears helped to reveal the presumptive diagnosis in all cases, which emphasizes the important role of direct microscopy in diagnosing pulmonary nocardiosis.
Our sixth patient is probably the first reported case in India who was retropositive and developed pleural effusion as well as pericardial effusion due to disseminated nocardiosis.
Although TMP-SMX is the drug of choice for Nocardia, the optimal drug therapy has yet to be established. CLSI guidelines state that all the isolates of Nocardia should be tested for multiple antimicrobial agents even though it may not always correlate with the clinical outcome. 6 In the present series, all of the isolated strains showed in vitro susceptibility to TMP-SMX. We had six cases treated with TMP-SMX alone, or in combination with a beta-lactam drug (cefepime, imipenem) or an aminoglycoside and all showed a favourable response with complete resolution. One patient who, after an initial good response had a relapse and was readmitted with altered sensorium, left against medical advice and therefore did not attend follow-up or treatment for dissemination. The probable cause might have been the in vivo resistance of Nocardia to the given treatment and dissemination of the infection to brain. Another patient died before the institution of specific treatment, which might have been due to the disseminated presentation of the disease on admission and late medical intervention.
Conclusion
Pulmonary nocardiosis is seen in immunosuppressed people with a post renal transplant or a pre-existing lung disease. Direct microscopy plays a key role in establishing the diagnosis from samples from pleural fluid, broncho-pulmonary aspirates and sputum. The early diagnosis of pulmonary nocardiosis leads to the prompt initiation of suitable treatment and, hence, a reduction in morbidity and mortality.