
Abstract
A total of 243 children aged one month to five years with World Health Organization defined severe community acquired pneumonia were studied for the presence of atypical bacterial pathogens: 24 were found positive for mycoplasma infection. There was no significant association with any of the clinical, laboratory and radiological variables in children with pneumonia by the atypical pathogen.
Introduction
Community acquired pneumonia (CAP) is a common infection that afflicts children throughout world. It is fundamentally different in children and adults. 1 Increasingly atypical bacteria (Chlamydia pneumoniae, Mycoplasma pneumoniae and Legionella pneumophila) are being associated with CAP in children. The importance of the atypical pneumonias is not related to their frequency (approximately 15% of CAPs), but to their difficulty of diagnosis and their non-responsiveness to recommended beta-lactam therapy. 2 Our study assesses the prevalence of these atypical bacterial pathogens in children aged one month to five years presenting with CAP. We also studied the relation, if any, between the presence of atypical bacterial pathogens and clinical, laboratory and radiological variables.
Patients and methods
The work was conducted in the Departments of Pediatrics and Microbiology at the Chhatrapati Shahuji Maharaj Medical University, Lucknow, India, from July 2005 to December 2006. Approval from the institutional ethics committee was obtained prior to starting the work. Children aged 1–59 months, admitted to the pediatrics ward with a clinical diagnosis of World Health Organization defined severe pneumonia, were included after we had obtained the informed written consent of parents or guardians. The sample size was calculated assuming ∼20% prevalence of atypical bacterial pathogens in CAP. In order to estimate this proportion with a 7% precision and an alpha level of 0.05, a minimum of 250 cases needed to be recruited. A structural questionnaire was prepared for interviewing the parent/guardian of the recruited children in order to discover the clinical symptoms and treatment history. Baseline laboratory and radiological parameters were abstracted from the hospital records.
Pneumonia was diagnosed when the children were admitted to hospital with cough or difficulty in breathing: an increased respiratory rate (IRR) or chest indrawing. IRR was defined according to age group as a respiratory rate of >60 breaths/min for children aged <2 months, >50 breaths/min for those aged two to <12 months and >40 breaths/min for those aged one to <5 years of age. 3
Two millilitres of blood was collected for immunoglobulin M (IgM) antibodies against C. pneumoniae by microimmunofluorescence (MIF) (Savyon Diagnostics Ltd, Israel) and M. pneumoniae IgM by enzyme-linked immunoadsorbent assay (ELISA: IBL, Germany). Nasopharyngeal aspirate was also collected at the same time by passing an infant feeding tube through each nostril: secretions were aspirated for antigen detection of M. pneumoniae by ELISA (Virion/Serion, Germany); bacterial culture of Legionella pneumophila (on buffered charcoal yeast extract [BCYE] obtained from Hi Media, Mumbai, India) and for polymerase chain reaction (PCR) for C. pneumoniae. 4
All kit-based tests were performed according to the manufacturer's instructions. For C. pneumoniae, an in-house PCR was done, using a pair of C. pneumoniae specific oligonucleotide primers CpnA and CpnB (Bangalore Genei Pvt Ltd, India) based on 16S r-RNA gene. The primer sequence is as follows:
CpnA 5′-TGACAACTGTAGAAATACAGC-3′ CpnB 5′-ATTTATAGGAGAGAGGCG-3′
Statistical analysis
Data was collected on predesigned questionnaire and then entered on a D-base. Analysis was done using software SPSS (11.0 version). Univariate distribution of variables was analysed. To assess the association between the presence of atypical infection and various clinical and laboratory radiological parameters, the chi-square test was used for categorical (discontinuous) variables and the students t-test was applied for continuous variables. A P value >0.05 was considered significant. Graphical representation of the monthly occurrences of cases of atypical pneumonia is shown in Figure 1.
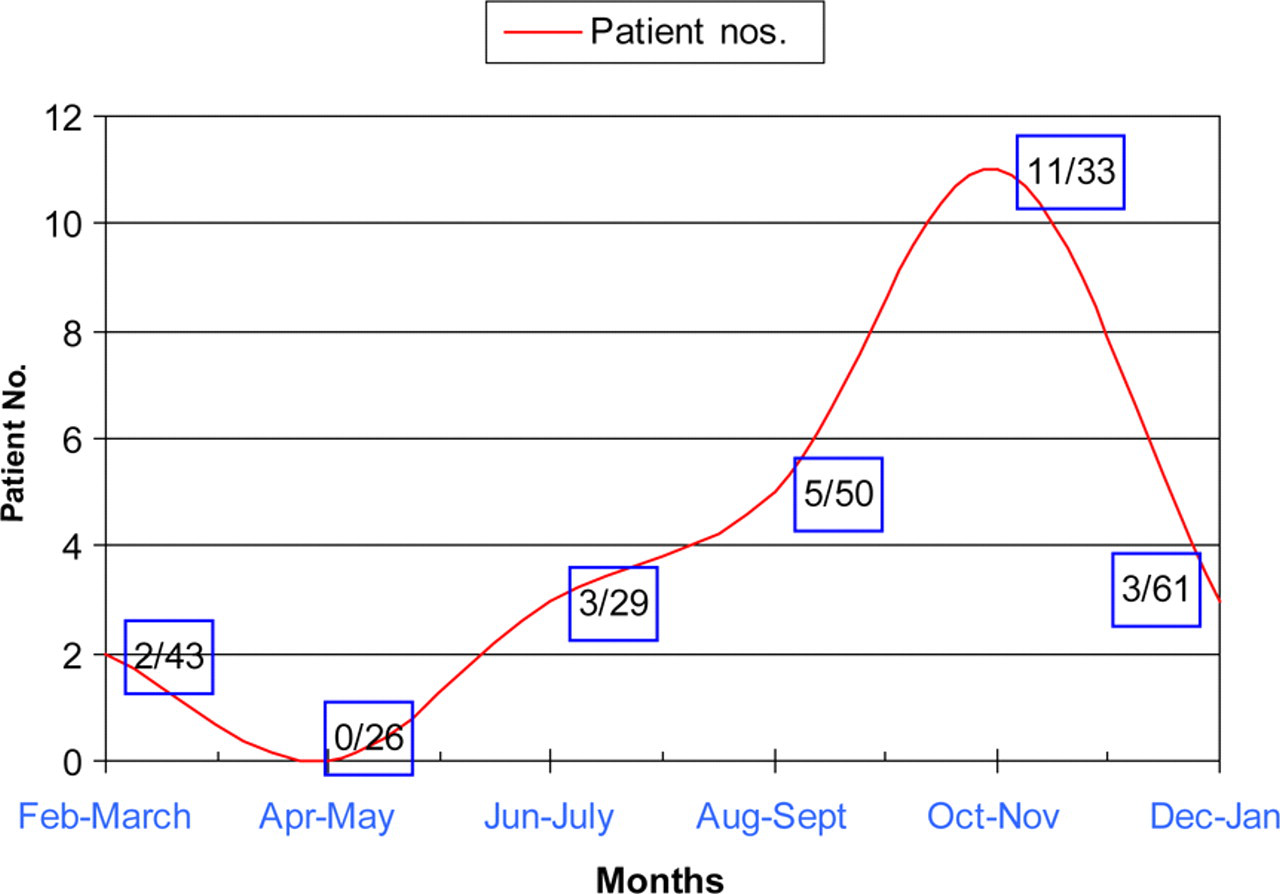
Monthly distribution of cases of mycoplasma infection. Numbers in boxes: the denominator is the total number of community acquired pneumonia cases in a two-month period and the numerator represents the number of cases positive for mycoplasma
Result and discussion
During the study period, 243 cases of CAP were recruited: 83 (34.1%) were girls; 73 were aged 1–2 months; 107 were aged 3–11 months; and 63 were aged 12–59 months. The mean age of the study population was 10.211 (standard deviation [SD] 12.903) months, mean weight 5.76 kg (SD 2.677) and mean height 63.921 cm (SD 12.4).
Of those recruited, 24 had an infection caused by an atypical bacterial pathogen. All cases had M. pneumoniae, 14 were positive by IgM antibody in serum and 10 by antigen ELISA in nasopharyngeal aspirate; none were positive for both. None were positive for C. pneumoniae by either PCR or by MIF assay; similarly none grew Legionella pneumophila on culture. Thus, the prevalence of atypical bacterial pathogens in children with CAP was 9.87% (24/243).
Eighty-eight (36.2%) presented in the months of December, January and February, although the yield of atypical pathogen was highest in October; nine of the 19 cases of CAP presenting in October had a mycoplasma infection (Figure 1). Although M. pneumoniae epidemics are less predictable, cases occurring in community-wide clusters during the winter have been reported. 5 The mean age, height and weight of the CAP cases with mycoplasma infection was no different from those negative for this pathogen. Most of the mycoplasma infection cases were aged 12–59 months. Of 63 cases of CAP in this age group, 11 had a mycoplasma infection. A history of antibiotic intake, previous hospitalisation, oxygen administration in the preceding six days and who lived in rural/urban areas did not show any statistical association with the presence of mycoplasma infection in the CAP cases. At the time of admission baseline symptoms, clinical signs, and laboratory and radiological parameters were recorded for all children. However, no unique differentiating features were found in those with CAP by atypical pathogens (Table 1). A clinical diagnosis of infection by atypical bacteria remains elusive as previously suggested. 6 The mean duration of hospital stay for children with CAP by mycoplasma was 8.74 days (SD 6.52) which was not significantly different from hospital stays for children not infected by mycoplasma.
A comparison of categorical variables in children with community acquired pneumonia
In the present study M.pneumoniae was found to play an important role in CAP affecting children up to the age of five years; C. pneumoniae was not associated with CAP in this age group. The higher prevalence of mycoplasma compared to chlamydia in children with CAP has been reported in a number of studies. 7 The available literature supports a low prevalence of C. pneumoniae infection in preschool aged children, i.e. <5 years, but it is an important cause of pneumonia among children over five years old. 8 In another study where four methods (cell culture, PCR, ELISA and MIF) were used for the diagnosis of C. pneumoniae infection, the authors found only a 1.2% positivity among admitted patients aged two months to three years. 9 Even in our previous work C. pneumoniae infection was found in only two of 73 children with CAP who were aged less than five years. 4 L. pneumophila infection in hospitalised children with community-acquired lower respiratory tract infections has been reported 10 but we did not find any cases of legionella infection. It has been reported that the majority of children with Legionnaires' disease have an underlying condition such as malignancy 11 but we did not find any such association in our study.