
Abstract
Endomyocardial fibrosis (EMF) was first described in 1948. It is an idiopathic disorder, characterized by the formation of fibrous tissue on the endocardial aspect of one or both ventricles, resulting in a restrictive cardiomyopathy with atrial enlargement. Originally described in Uganda, numerous cases have also been described in the Middle East.
Case history
A 60-year-old Ugandan man requested a second opinion regarding his cardiovascular condition. He had been given a diagnosis of hypertensive heart disease in Paris, France. At the time of consultation he had been suffering from dyspnoea, peripheral oedema and palpitations for a period of approximately five years, with a marked increase in peripheral oedema and dyspnoea over the previous six months. He was taking furosemide 80 mg mane and 40 mg nocte, spironolactone 100 mg mane, ramipril 5 mg mane, aspirin 100 mg mane and digoxin 0.25 mg mane, as prescribed by the clinician in France.
Clinical examination revealed a clinical picture of severe biventricular, congestive heart failure with atrial fibrillation (AF). The AF was confirmed by electrocardiography.
Transthoracic echocardiography revealed a massively enlarged left atrium, measuring 9.65 cm in diameter (Figure 1) and a non-dilated, hypertrophic left ventricle (Figure 2). The apical, four-chamber view (Figure 3) revealed a classic picture of endomyocardial fibrosis with massively enlarged atria (the right atrium measured 13 cm in diameter), non-dilated ventricles and shrunken papillary muscles and chordae tendineae with severe atrioventricular valvular regurgitation.
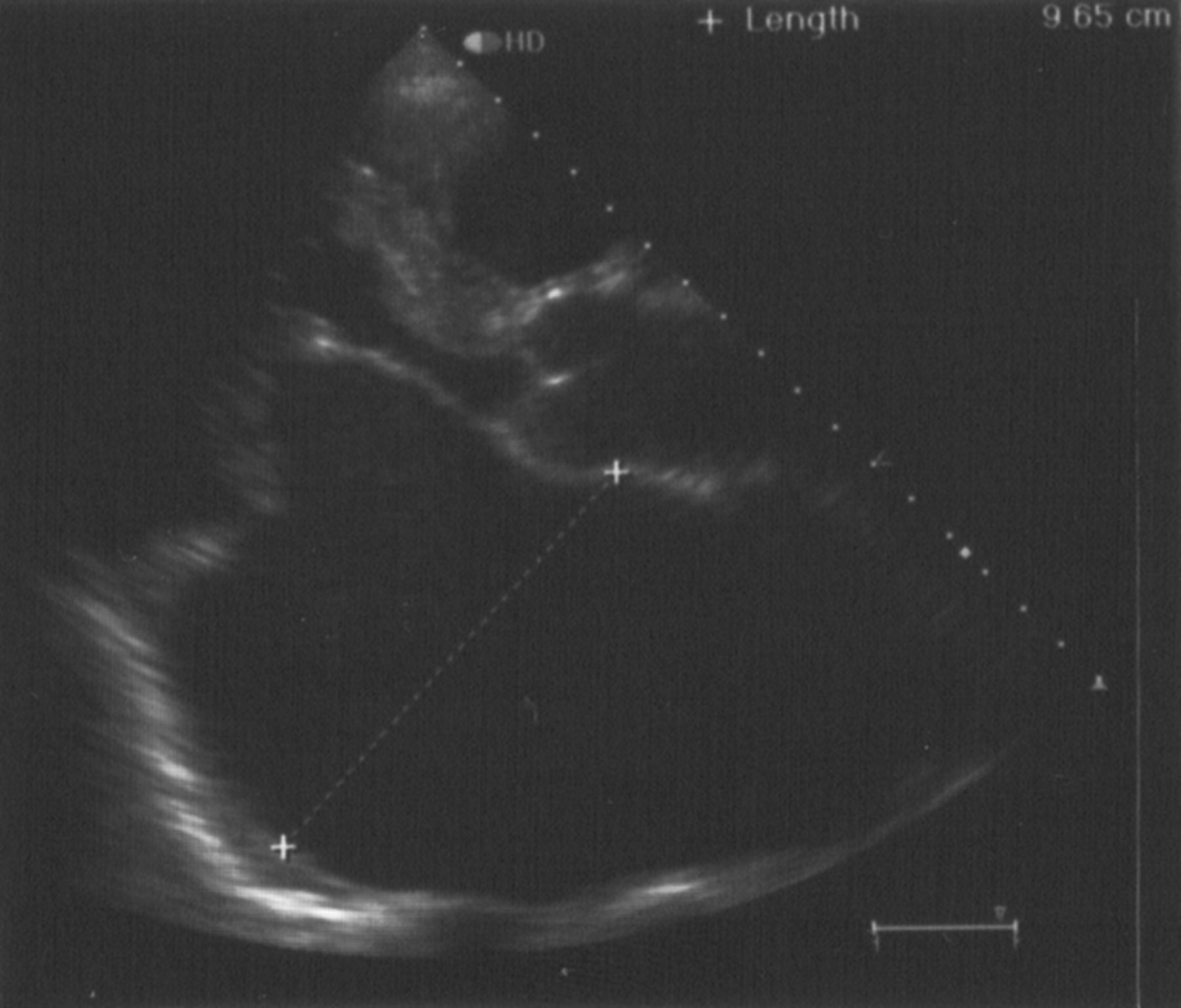
Parasternal, long-axis view, demonstrating a massively enlarged left atrium
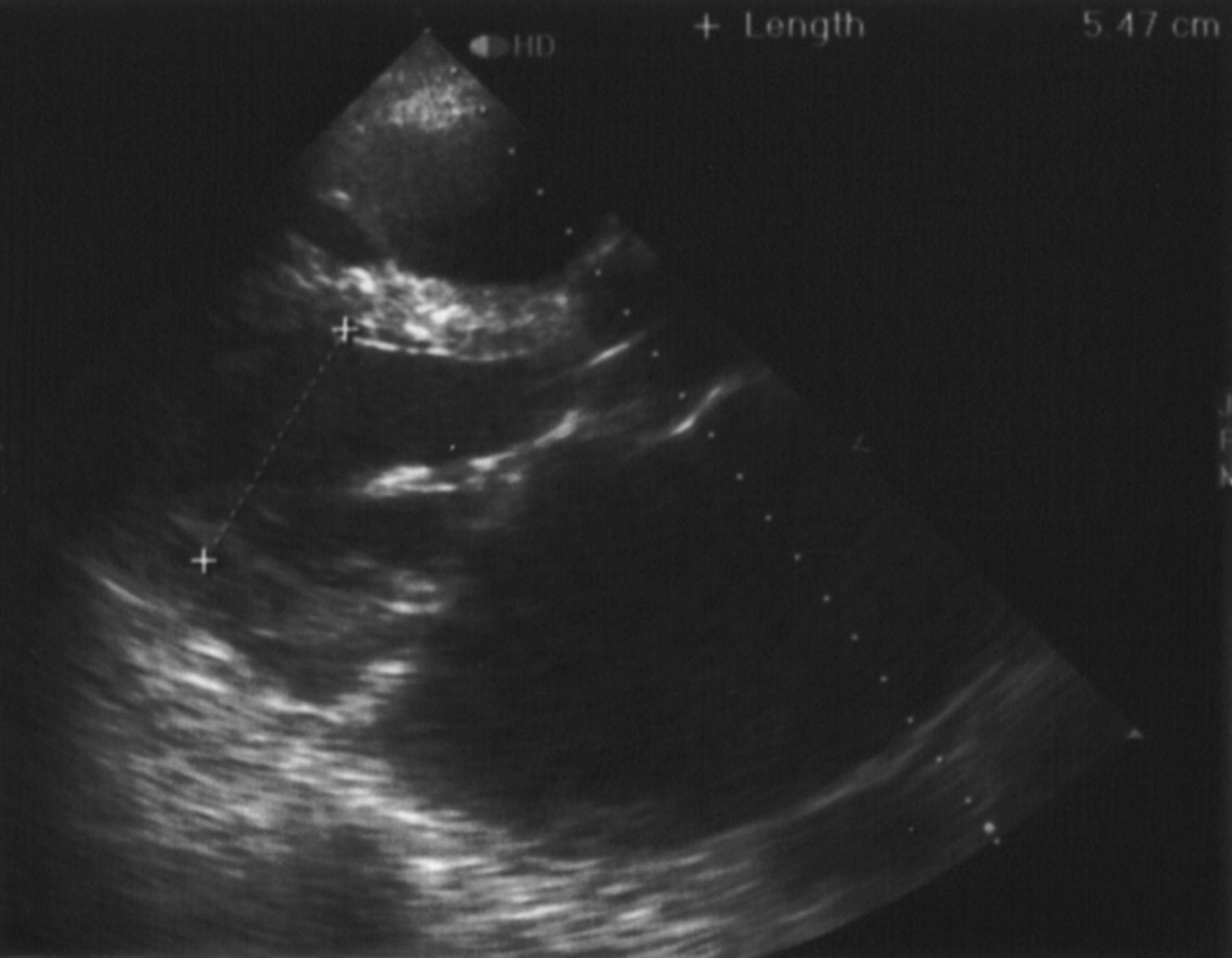
Parasternal, long-axis view, demonstrating a normal left ventricular end-diastolic diameter, thus excluding dilated cardiomyopathy
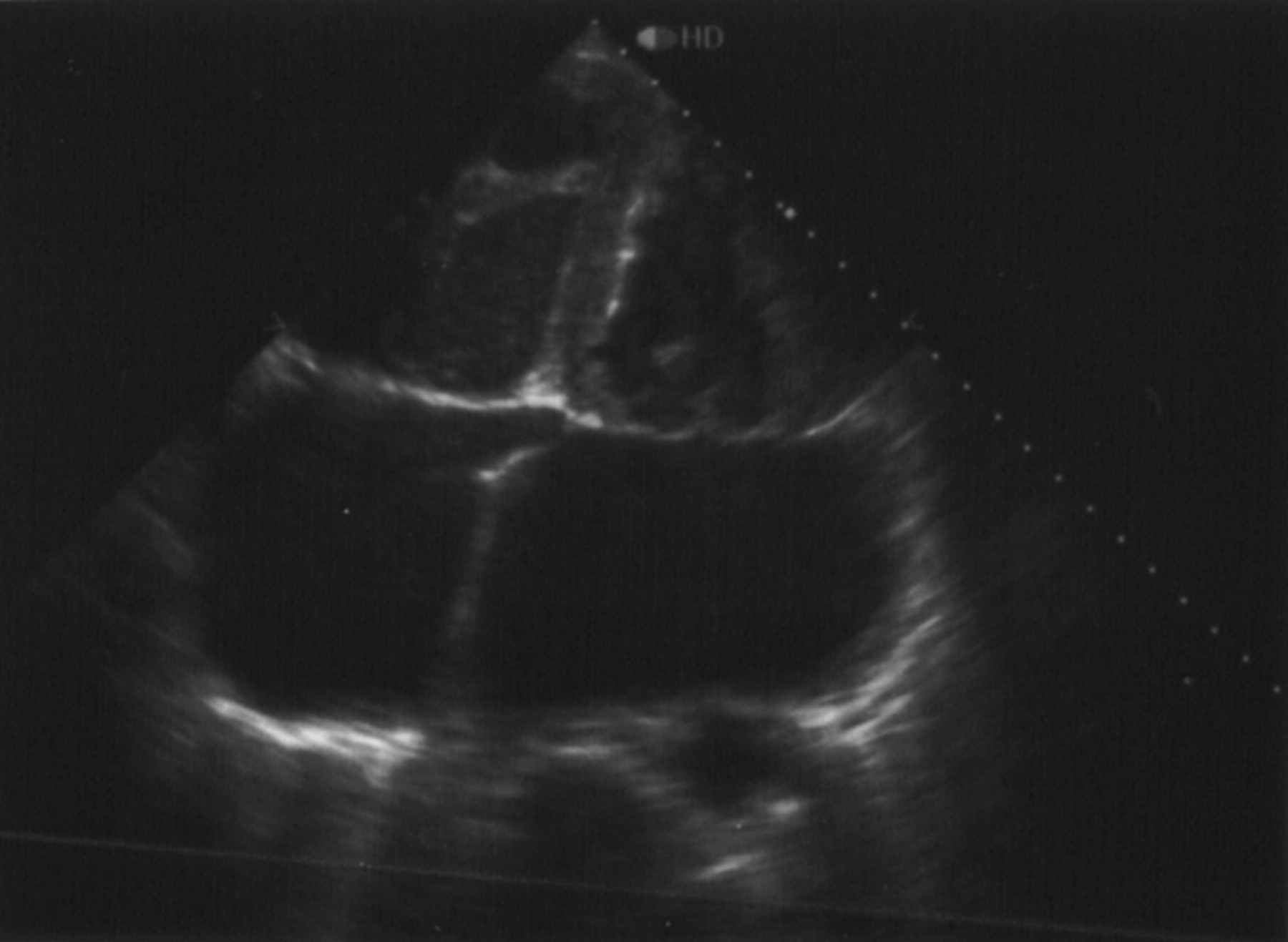
Apical, four-chamber view, demonstrating the classic echocardiographic appearance of endomyocardial fibrosis. Note the massive enlargement of both atrias with small ventricles
The patient declined surgery and warfarin was subsequently added to his therapeutic regimen.
Discussion
This case illustrates the importance of excluding mimics of hypertensive heart disease. Relying only on the parasternal, long-axis view (Figures 1 and 2) the combination of a dilated left atrium with a hypertrophic, non-dilated left ventricle led to the erroneous impression of hypertensive heart disease. However, the apical, four-chamber view (Figure 3) illustrates the classic echocardiographic appearance of endomyocardial fibrosis.
The essential feature of endomyocardial fibrosis (EMF) is the formation of fibrous tissue on the endocardial aspect of one or both ventricles. 1 This fibrotic process involves the apex, inflow tract and papillary muscles of the affected ventricle. 1–3 This results in rigidity of the endocardium, progressive reduction in the cavity of the involved ventricle and severe atrioventricular valve incompetence. 2–5
EMF is responsible for approximately 25% of all cases of congestive heart failure in equatorial Africa. 2,6 However, the disease has also been well described in the Middle East 2 and in India, Brazil, Colombia and Sri Lanka. 7
EMF is most common in black children, but is known to afflict individuals into the sixth decade and white subjects in temperate climates. 1–7
Clinically EMF has many mimics, notably constrictive pericarditis, rheumatic heart disease, the apical variant of hypertrophic cardiomyopathy, apical thrombus and Ebsteiǹs malformation of the tricuspid valve. 2 A rare mimic of right-sided EMF is Behcet̀s disease where obliteration of the right ventricular apex by clot may occur without tricuspid regurgitation. 2,8
The echocardiographic picture of normal-sized ventricles with hugely dilated atria should cause one to suspect EMF. This combination will help in the exclusion of mimics of EMF
2
such as: Rheumatic valvular regurgitation, where the involved ventricle will be dilated; Constrictive pericarditis and Behcet̀s disease with normal sized atria dilated cardiomyopathy, where huge atria will be accompanied by dilated ventricles.
Apical obliteration is characteristic of EMF and can be distinguished from the apical variant of hypertrophic cardiomyopathy, where apical obliteration occurs only in systole.
2
Echocardiography is essential for the diagnosis of EMF—a fascinating disease with an as yet unknown cause—and endomyocardial biopsy is not necessary. 2