
Abstract
The case records of 202 consecutive adult Nigerian in-patients with stroke at the University of Port Harcourt Teaching Hospital (UPTH) were retrospectively reviewed. The mean age at presentation was 62.62 ± 14.2 years. The male to female ratio was 1:1.2. The commonest risk factors were hypertension, diabetes mellitus, hypercholesterolaemia, older age and a previous history of stroke. Clinically, 67.3% had cerebral infarction (CI), while 27.7% had intracerebral haemorrhage (ICH). The peak age of events for both sub-types was the 7th decade. The case fatality was 55.4% for ICH and 23.5% for CI. Thus, stroke is associated with high mortality at the UPTH. Improved emergency care of stroke patients is needed while the setting up of dedicated stroke centres is advocated. A community-based study is necessary to provide more insight into the problem and also highlight the basis for appropriate intervention and policy.
Introduction
In sub-Saharan Africa, where infectious diseases remains the leading cause of death, hypertension and stroke are emerging as important causes of morbidity in the rapidly urbanizing population of the region. 1 Nigeria's modest economic development coexists with poverty, malnutrition and high maternal and child mortality rates. Paradoxically, poverty and affluence may both bring disease. Specifically, there is an inverse relation between birth weight and cardiovascular disease (CVD) in later life. 2 Higher income black Africans are more susceptible to CVD than high-income white or other non-black Africans. 3 Thus, whether poor or rich, CVD (stroke inclusive) is a major burden for black Africans.
This study reviewed the age, sex incidence, risk factors, stroke subtypes and case fatality of stroke over a three-year period at the University of Port Harcourt Teaching Hospital (UPTH).
Materials and methods
The UPTH is a tertiary health institution situated in Port Harcourt, capital of the Rivers State in the Niger Delta Basin of Nigeria. The records of all patients admitted to the medical wards over a three-year period (Jan 2003 – Dec 2005) were studied. Those with a clinical diagnosis of stroke were reviewed. Demographic and clinical data were extracted from the records.
Only those who had complete information and met the World Health Organization (WHO) criteria for the clinical diagnosis of stroke were included. An attempt was made to classify the patient into stroke subtypes on clinical grounds using the WHO criteria.
The procedures followed were in accordance with UPTH institutional guidelines and the hospital ethical committee approved the study. Data was analysed using SPSS11 statistical package.
Results
Over a three-year period, 26,505 patients were admitted to the hospital with 2178 (8.2%) being medical admissions. A total of 202 patients were diagnosed to have stroke. This constituted 9.3% of all medical and 0.76% of all hospital admissions. The ages ranged from 25 years to 115 years with a mean of 62.61 ± 14.2 years. The peak age was in the seventh decade (Figure 1). There were 93 men and 109 women, giving a male:female ratio of 1:1.2.
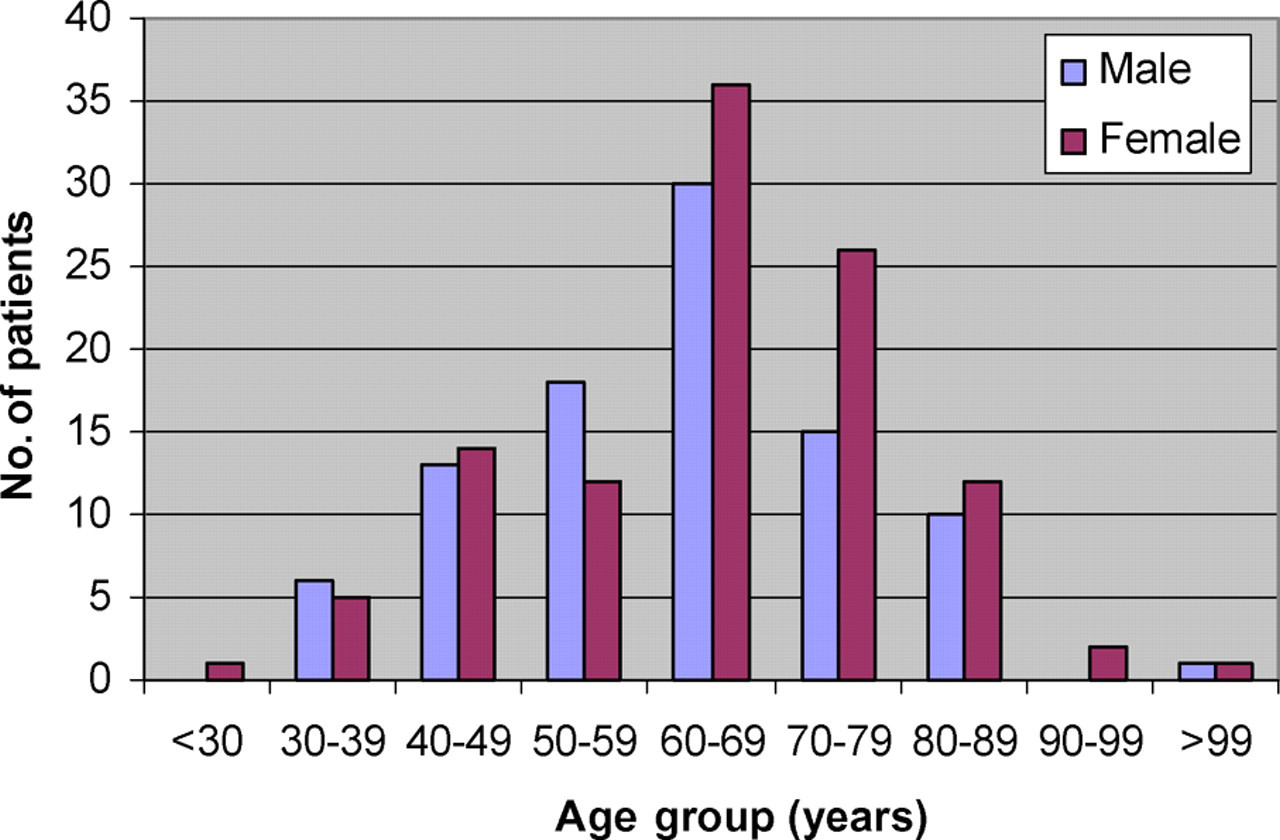
Age-sex distribution of patients with stroke
The predisposing risk factors among the stroke patients were: hypertension 90.5%; diabetes mellitus 24.4%; hypercholesterolaemia 10.1%; excessive alcohol intake 7.7%; and obesity 6.5%. Atrial fibrillation, cigarette smoking and human immunodeficiency virus (HIV) infection were found in 0.6 % of the stroke patients. Twenty-three patients (13.7%) had suffered a previous stroke.
Of the 202 patients, 136 (67.3 %) had cerebral ischaemia (CI) and 56 (27.7%) had intracerebral haemorrhage (ICH). Five (2.5%) had subarachnoid haemorrhage and five (2.5%) had ICH with sub-arachnoid extension (Table 1). The peak age of both ischaemic and haemorrhagic stroke was at the seventh decade (60–69 years).
The distribution of stroke subtype, outcome and age group
DAMA, discharged against medical advice; F, female; M, male
Of the 93 men, 33 (35.5 %) died and four (4.3%) discharged themselves against medical advice. Fifty-six (60.2%) were discharged home to continue with outpatient rehabilitation. Of the 109 women, 34(31.1%) died, 71 (61.5%) were discharged, three (3.7%) discharged themselves against medical advice and one (0.9%) absconded (Table 1). The case fatality rate for CI was 23.5%, and for ICH it was 55.4% (Table 1).
Discussion
This study showed that stroke constituted 9.3% of all medical admissions at the UPTH. This is similar to the 8.7% of medical admission at Ogun State University Teaching Hospital (OSUTH). 4 The relative predominance of women in this study differs from the findings in some other reports from Nigeria, 5,6 but is similar to that of Ogun et al. 7 Male gender is a recognized risk factor for stroke. 10 Our patient series, like many others in Nigeria, is hospital-based and therefore does not represent an adequate epidemiological sample.
Hypertension constituted the highest risk factor (90.5%) for stroke in this series. This high figure may be due to the ignorance of the natural course of hypertension, self-denial of the illness, limited access to medical care and poor drug compliance. Both diabetes mellitus and hypercholesterolaemia were among the four main risk factors for stroke, with a frequency of 24.4% for diabetes. Therefore, any strategy which aims to limit the incidence of stroke in Port Harcourt and, indeed sub-Saharan Africa, must be interventional. There must be public awareness campaigns, adequate and regular treatment of hypertension and life style modifications.
Obesity appears currently limited to a specific segment of sub-Saharan Africa, 8 particularly those whose life style has become very westernized. The 7.65% prevalence of obesity among the stroke patients studied was low. While obesity is emerging as a new health problem, malnutrition still remains a serious public health problem in sub-Saharan Africa. This is exacerbated by the burden of HIV/AIDS on families, by famine and by political conflicts. 8 These could contribute to the low prevalence of obesity in this study.
Malnutrition and infection as risk factors for stroke in Africans has been established. Malnutrition by predisposing populations to infection constitutes a risk factor for stroke in patients with sickle cell disease and in childhood. 9 The interaction between infection, malnutrition, westernization and obesity and the causes of stroke need to be studied further.
HIV infection as a possible cause of stroke was seen in 0.62% of our patients. With the increasing incidence of HIV infections in Nigeria and sub-Saharan Africa, there may be a need to determine the HIV status of all stroke patients as it may present with treatable stroke-like conditions such as tuberculomas, brain abscesses and central nervous system toxoplasmosis. Approximately 14% of our patients had a history of previous stroke which may be a reflection of inadequate secondary prevention.
In our study there was a predominance of CI (67.3%) which is similar to findings from other centres in Nigeria. These results should be interpreted with caution as stroke sub-type in all these centres, including ours, was diagnosed clinically. Appropriately timed computerized tomography scans remain the gold standard for the diagnosis of stroke sub types.
The case fatality in this study of 33.1% was high although lower than the 50% recorded at OSUTH. 8 Cerebral haemorrhage with a case fatality rate of 55.4% is still a more common cause of fatal stroke. The high stroke case fatality rate seen in Nigeria may be due to limited stroke rehabilitation services and poor infrastructural facilities for stroke management. Extracerebral complications such as bed sores, frequent use of indwelling catheters, chest infection, inadequate nursing and physiotherapy and a paucity of drugs may all contribute to the high mortality rate. 10
Improved emergency care of stroke patients is needed. People should be educated about the early signs of stroke so that they go to hospital in time. Dedicated stroke centres should be set up as this has been found to reduce stroke mortality. 7
Conclusion
Stroke remains a common problem in Nigeria. Hypertension, diabetes mellitus and hypercholesterolemia are the main risk factors. Cerebral ischaemia is the most common stroke subtype. It is recommended that hypertension control and screening programmes for diabetes mellitus and hypercholesterolaemia be established.