
Abstract
Spontaneous small intestinal perforations are common in India. Surgeons operating on patients with an obscure peritonitis should be aware of the diverse aetiologies of small intestinal perforations in order to be able to provide the appropriate management. We reviewed the pathology records of 165 patients operated on for nontraumatic perforations of the small intestines in our hospital between 2005 and 2007. Perforation edge biopsy was diagnostic in 53 cases, with typhoid being the most common aetiology, followed by TB. The majority of cases, however, revealed only a non-specific inflammatory granulation tissue. However, the sensitivity of biopsy diagnosis could be increased by taking additional biopsy material from the mesenteric lymph nodes, tubercles or omental nodules. We conclude that perforation edge biopsy is useful in a third of cases, but the diagnostic rate could be improved by taking additional biopsy material.
Introduction
Surgeons operating on patients with obscure peritonitis need to be aware of the diverse aetiologies of small intestinal perforations. In developing countries, perforation peritonitis is a common surgical emergency. Ulcer/perforation edge biopsy is taken routinely to establish a diagnosis and to aid the clinical management of the patient. Preoperative aetiologic diagnosis is usually not possible at the time of the exploratory laparotomy. Postoperative treatment is often based on histological reports which may not be contributory in a significant number of cases. In view of the significant number of intestinal perforation cases admitted to our institute, we carried out an investigation into the diagnostic difficulties encountered. The present study is a retrospective review of the biopsy specimens of 165 patients diagnosed in the emergency room with perforation peritonitis due to small bowel perforation, in order to evaluate the role of perforation edge biopsy in establishing the aetiology of perforations.
Patients and methods
Ulcer edge biopsies of the small bowel, submitted to the Department of Histopathology, University College of Medical Sciences and GTB Hospital, Shahdara, Delhi, during 2005–2007 (three years) were included in the study. Segments of intestines removed during similar emergency procedures were excluded from the study. All the biopsies were taken in the emergency operating room and had no preoperative diagnosis. The biopsies were formalin-fixed and paraffin-embedded. Routine haematoxylin and eosin-stained sections were available in all cases and special stains were performed whenever required.
Results
There were 165 patients: 122 (74%) males and 43 (26%) females with a male:female ratio of approximately 3:1. The median age of patients was 25 years (range 1.5 years to 75 years) (Figure 1). Clinical symptoms of abdominal pain, vomiting, constipation and abdominal distension were seen in the majority of patients. Radiological findings were available in all cases at the time of surgery and included gas under diaphragm and air-fluid levels. The perforations were found in the terminal ileum in most cases. Only seven patients had a perforated jejunum, including two with multiple perforations involving both the jejunum and the ileum.
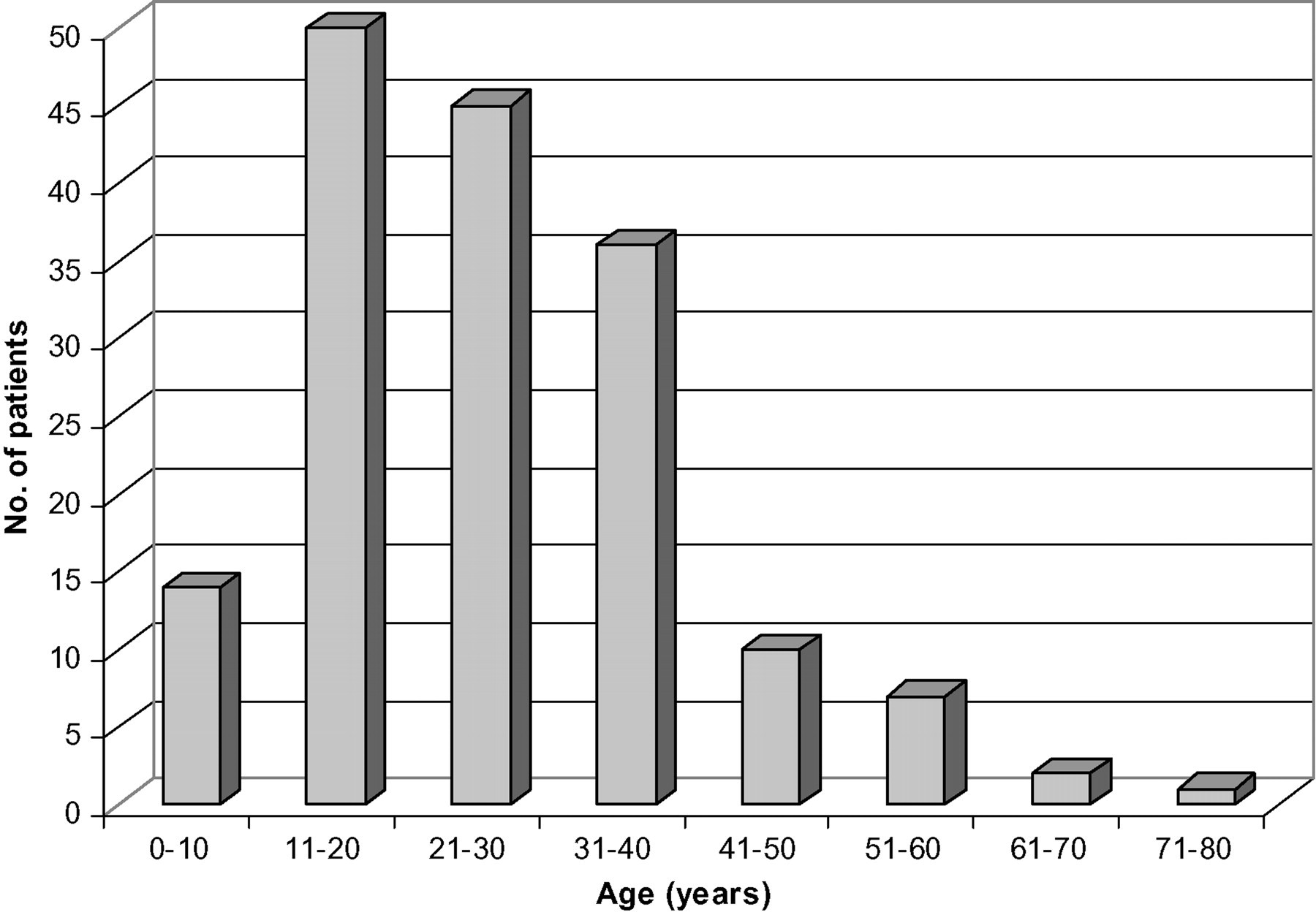
Age distribution of 165 cases of small intestinal perforations
A histological review revealed a definite histological diagnosis in 53 (32%) cases. The majority (n = 112) were described as non-specific inflammatory granulation tissue (Figure 2) and serositis with evidence of perforation peritonitis. Among the cases diagnosed as having a definite pathology for perforation edge biopsy, typhoid (Figures 3 and 4) was the most common diagnosis followed by TB (Figures 5 and 6; Table 1). One case of metastatic adenocarcinoma was also identified (Figure 7). Additional biopsy specimens were submitted in 10 cases (eight lymph nodes and two tubercles). The eight lymph nodes were diagnosed as tuberculous lymphadenitis (four cases), typhoid granulomas (two) (Figure 8) and reactive hyperplasia (two). Both tubercles were confirmed as being granulomatous inflammation with caseation upon histology. Only 2/10 cases of additional biopsy specimen had a definite diagnosis (TB) after perforation edge biopsy. The definite diagnoses available thus increased from 53 cases (32%) to 59 (38%) (apart from two reactive lymph nodes) by including additional biopsy material for the study. Thus, sensitivity of diagnostic perforation edge biopsy was improved by submitting additional biopsy material.
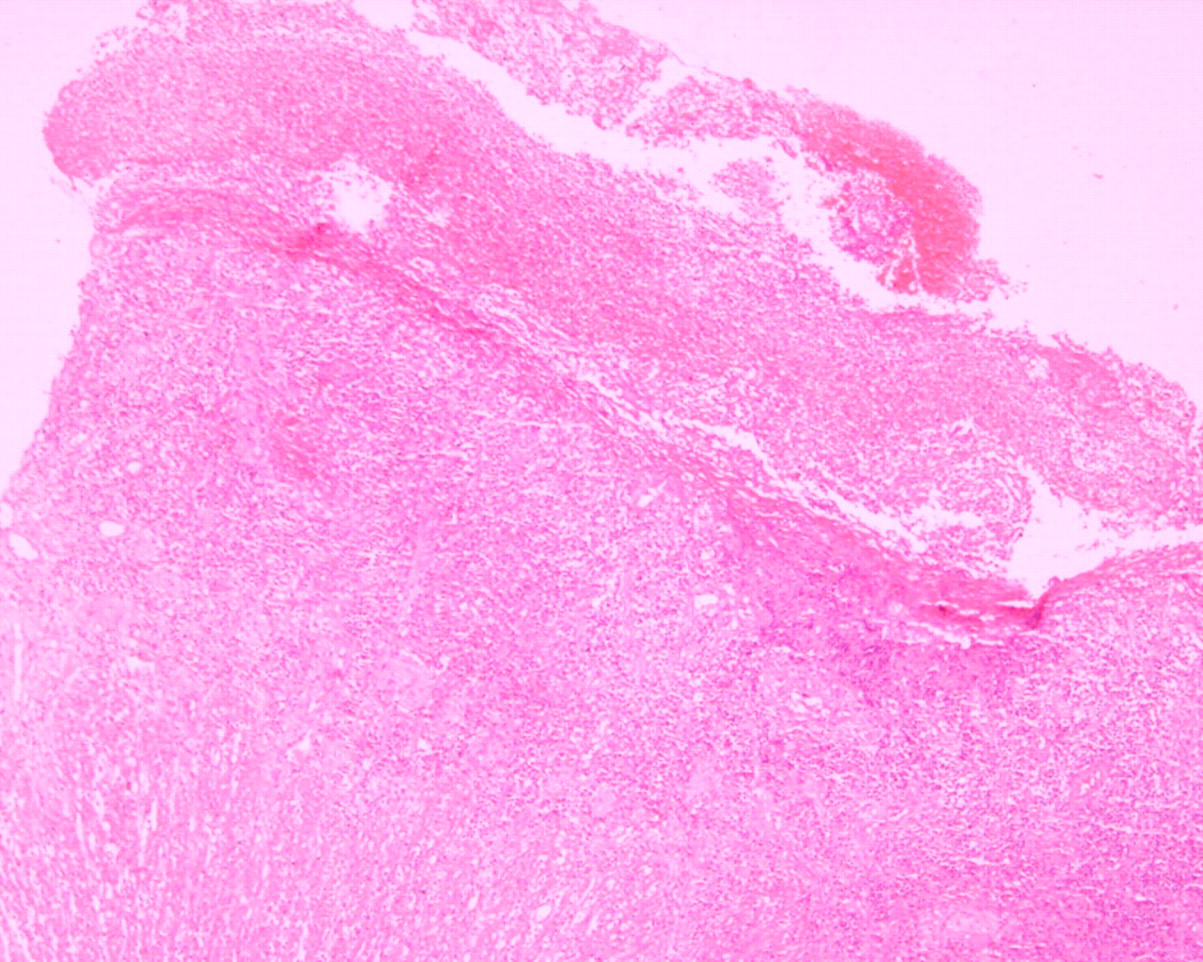
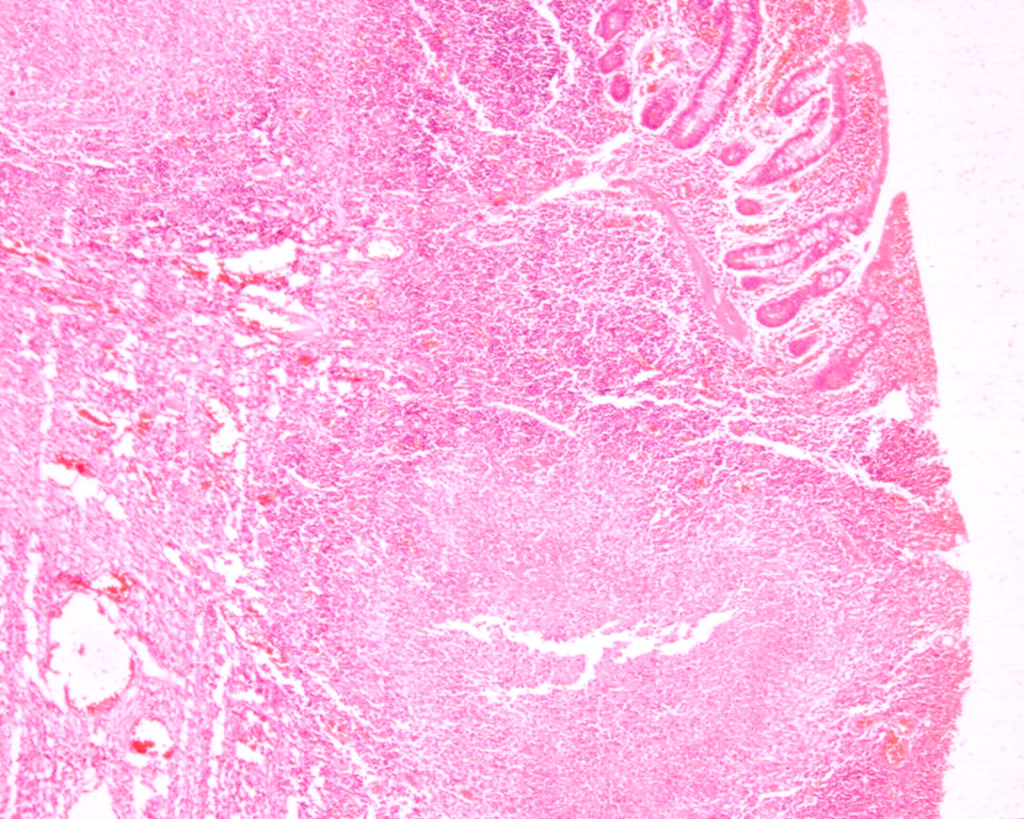
A scanner view of a non-specific ulcer edge biopsy showing a fibrinopurulently lined ulcer margin with underlying inflammatory granulation tissue (H&Ex 40)
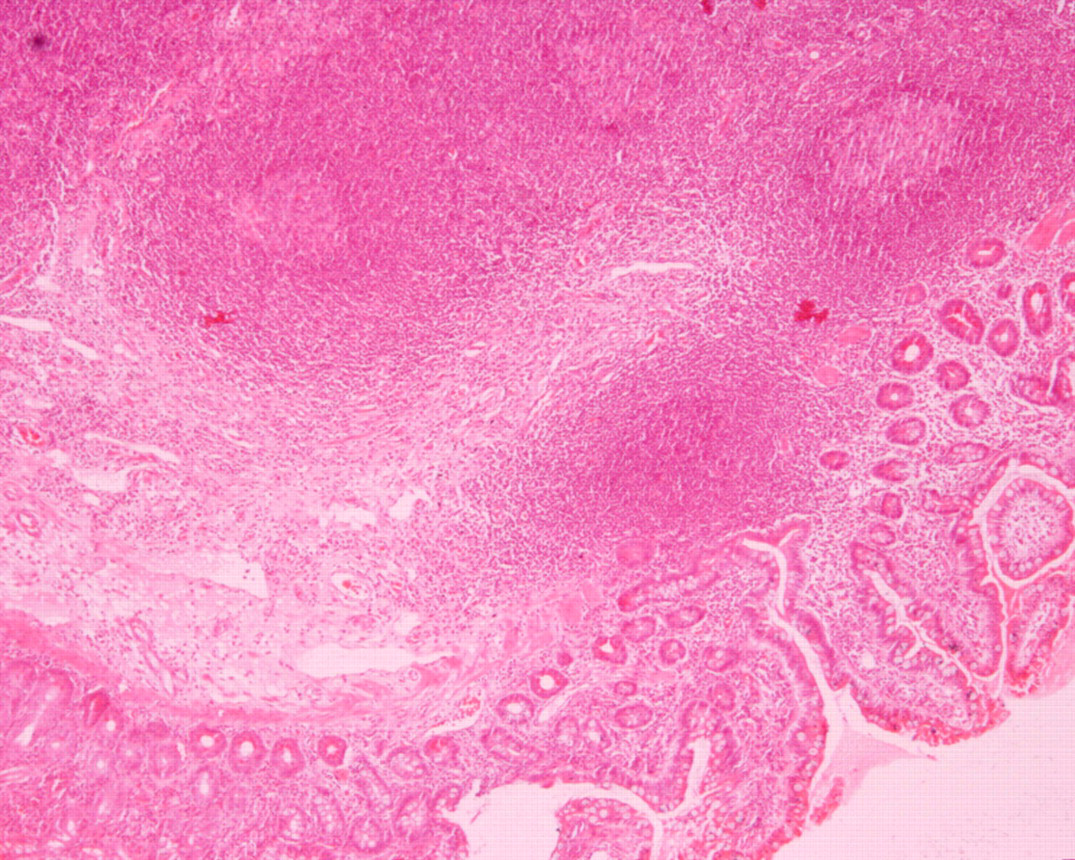
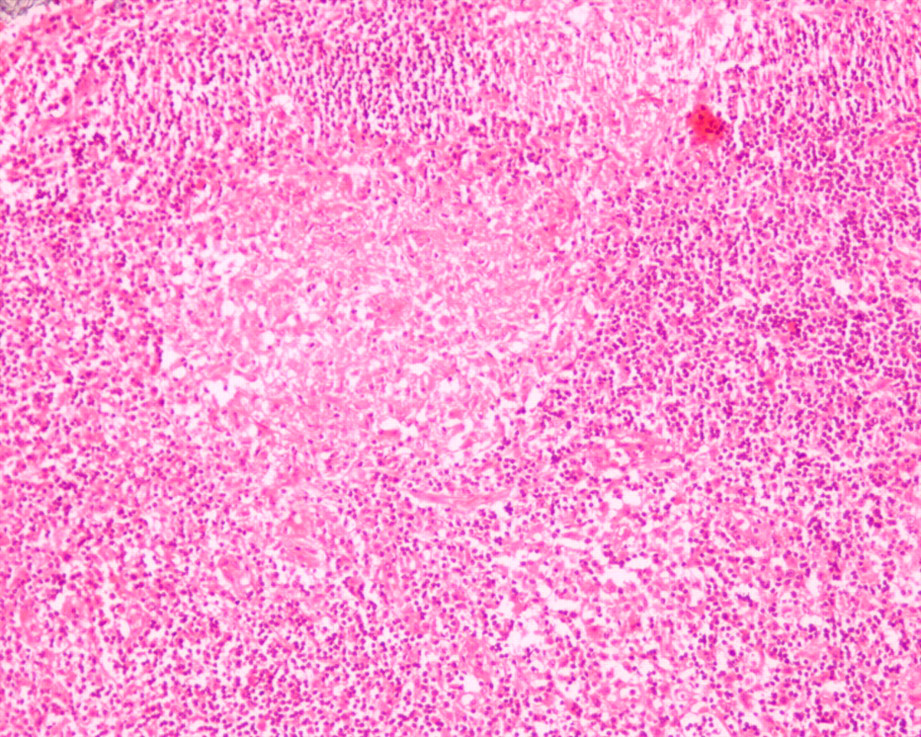
A scanner view of typhoid perforation edge biopsy showing dense lymphoid hyperplasia in submucosa (H&Ex 40)
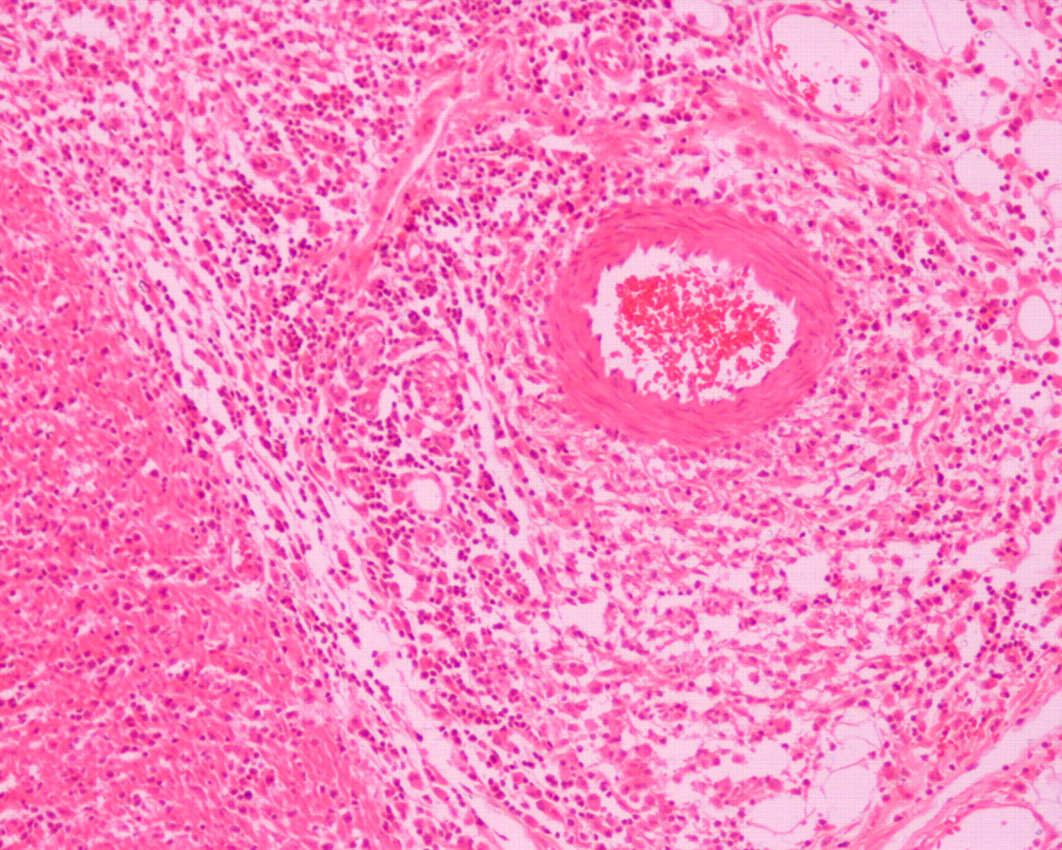
Higher power view of perivascular typhoid granuloma in a perforation edge biopsy (H&Ex 100)
A scanner view of perforation edge biopsy showing epithelioid cell granuloma with central caseous necrosis, diagnostic of TB
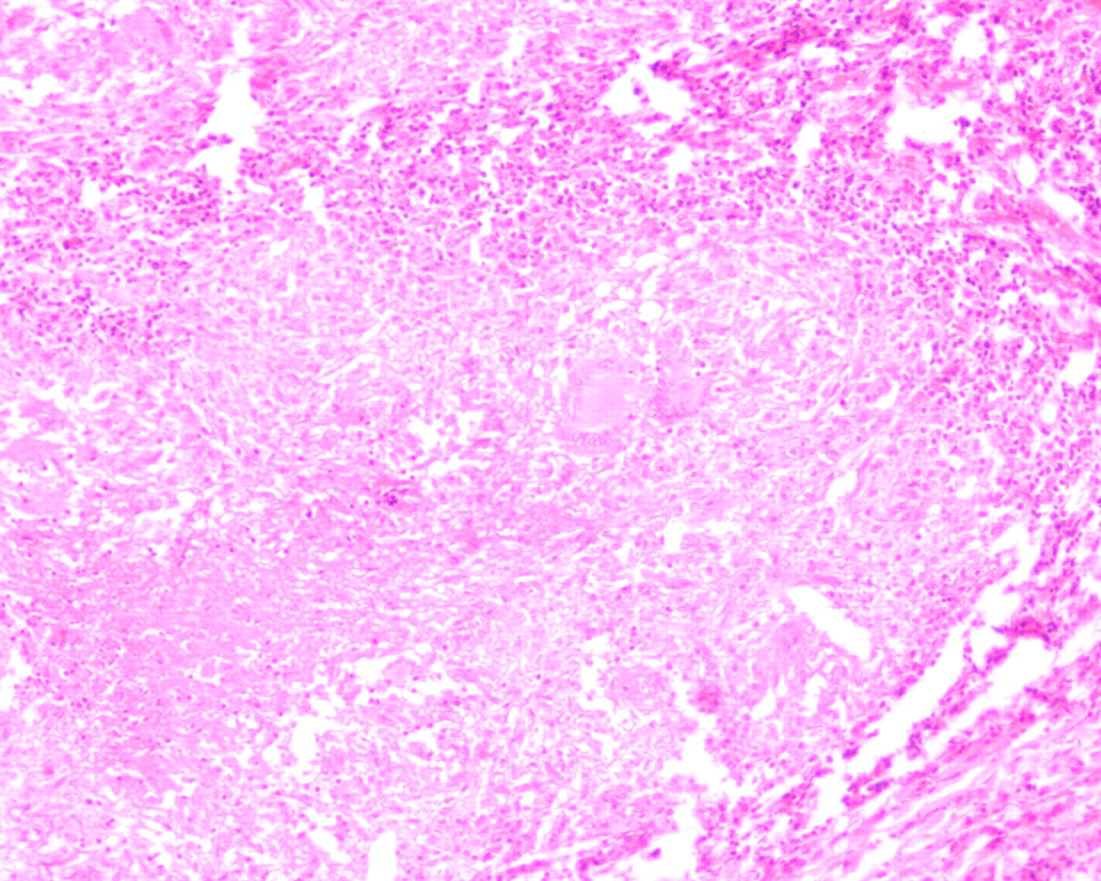
Higher power view of same showing epithelioid cell granuloma, langhans' giant cell and caseous necrosis (H&Ex 100)

A section showing a biopsy taken from a perforation due to metastatic adenocarcinoma (H&E x 40)
A section taken from the mesenteric lymph node showing typhoid granuloma (H&Ex 100)
Histological diagnosis of perforation edge biopsies
Discussion
The definition of nontraumatic perforation of small intestine (NTPSI) excludes perforated duodenal ulcers and perforation due to external hernias and primary ischaemic events. The mortality of 15–39% is attributed by some authors to nonspecific clinical presentations with a resultant delayed diagnosis. 1–4 In most series the clinical picture is non-specific. There is usually a moderate localized or generalized tenderness but not a board-like rigid abdomen as in cases of gastric or colonic perforations.
NTPSI is a rare entity in western literature. 1 The data from this study demonstrates that: NTPSI is quite frequently seen in our region; occurs in all age groups; and may be a manifestation of many unidentified causes. A perforation of the small bowel seems to be more common in elderly patients in western studies. In a large study from Sweden by Leijonmarck et al., only 17/112 patients were younger than 50 years old. 1 In our study the majority of patients were young adults. This may be due to a difference in aetiology of perforation in our study and the western literature where ingested foreign bodies, radiotherapy, diverticula, ischaemia, etc., are the main causes. 5 In other studies from the developing world, primary infections such as typhoid fever and TB are the main causes of NTPSI. Leijonmarck et al. also observed a great difficulty in making a correct diagnosis preoperatively. Most of their perforations also occurred in the distal ileum, making the mistaken preoperative diagnosis of appendicitis the most common complaint.
Typhoid and TB were the main causes in which the aetiology could be established by histopathology in our study. However, in the majority of cases, no aetiological factor was apparent on the biopsy specimen of intestinal perforation and so they were reported as ulcers of non-specific aetiology. Waisberg et al. also ascribed ulcers of nonspecific aetiology as the most frequent cause of intestinal perforation. These ulcers were not associated with any identifiable underlying disease and were frequently found in the ileal areas. Though mostly described single ulcers, there were many cases of multiple ulcers. 6
The histopathological examination of these non-specific ulcers shows that the ulcer base is formed by granulation tissue and fibrino-purulent exudate; the arterioles show fibrosis of the intima layer and maybe occluded. However, a nonspecific diagnosis can still not rule out the possibility of TB or typhoid from these biopsies as a consequence of focal involvement of the disease.
Perforation is one of the most lethal complications of typhoid fever, arising from necrosis of the Peyer's patches in the terminal ileum. Although the mortality due to typhoid perforation has decreased slightly over the past decade, it still ranges from between 9% and 50% with surgical intervention and over 40% with conservative management. 7,8 Typhoid ileal perforation commonly affects young adults in the second and third decade of the life which concurs with our results. It is more common in males, and a possible explanation could be that males spend more time in outdoor activities, and eat outdoors more often. 9
The complications of bowel TB requiring surgical intervention are: bowel obstruction; peritonitis; gastrointestinal haemorrhage; fistula formation; and intestinal perforation. 10–12 Acute perforation of a tuberculous ulcer is uncommon because of the reactive thickening of the peritoneum and the formation of adhesions with surrounding tissues. 13 The reported incidence of free perforation in TB is 1–10%. 11,13 An increased incidence of perforation has been observed in patients taking antituberculous chemotherapy. This is presumably due to a reduced inflammatory response which leads to the poor healing of ulcers and a reduced tendency of reinforcement by the mesentery. 14,15 Although perforation may occur in any part of the bowel, the distal ileum appears to be the most common site. In 90%, the perforation is solitary and a stricture is almost always present just distal to the perforation. 16,17 Multiple perforations are associated with a poor prognosis.
Chaikof et al., in their study of series of NTPSI, found 17 perforation cases caused by malignancy, of which 12 were metastatic. 3 We found only one case of metastatic adenocarcinoma leading to perforation (it was not suspected at the time of laparotomy). We did not encounter any primary small bowel malignancies presenting with acute perforation which had just been sampled and repaired.
Abdominal TB and typhoid are usually accompanied by enlarged mesenteric lymph nodes and peritoneal tubercles (in TB). Because these are the draining lymph nodes, the chances of finding an active disease in the mesenteric lymph nodes are very high, even if biopsy edge is noncontributory. An active lookout for these can be of help in reaching a histological diagnosis for a significant number of cases. Surgeons should be made aware that sampling these additional materials will improve the diagnostic worth of the biopsy material.
We did not encounter any studies based on the histological review of small bowel perforation margin biopsy. Other authors have, however, also commented on the difficulty of getting a definite diagnosis from perforation edge biopsy reports. 6 TB and typhoid are the most common causes of NTPSI in the developing countries and a high index of suspicion is essential for the early diagnosis and optimal treatment of such cases. This is particularly important in patients who present with non-specific abdominal symptoms and those who develop acute abdominal pain while receiving therapy for TB or enteric fever. Perforation edge biopsy is a useful tool for aiding the doctor to reach a definite diagnosis and, thus, can be a useful aid for the appropriate management of the patient. Additional sampling of omental nodules, lymph nodes and tubercles would be contributory, and would definitely reduce the number of cases signed out as perforation of unknown aetiology which are included in NTPSI.