
Abstract
Mediastinal mass is not an unusual entity. It occurs mostly due to lymphoma, thymoma, germ cell tumours, granulomatous diseases, and so on. Tuberculosis is an uncommon cause of mediastinal mass. It is rarely suspected when it is presented in such an unusual way. We report here a case of a 35-year-old male who presented with mediastinal mass, which was later confirmed as a case of tuberculosis on histopathological examination. He was successfully treated with anti-tubercular drugs.
Introduction
Tuberculosis is a disease which may present with atypical or unusual features; this sometimes causes problems in its diagnosis. Here, we report a case in which tuberculosis is presented as a mediastinal mass.
Case history
In May 2007, a 35-year-old male, non-smoker presented with complaints of chest discomfort occurring for the last three months. He had lost approximately 5 kg of his weight within the last two months. However, there was no history of shortness of breath, haemoptysis or fever. His vital signs were within normal limits. The neck veins were not distended, and no peripheral oedema, clubbing, or cyanosis was present. Chest movement and air entry was bilaterally equal in all the areas of chest, except for the right parasternal area where breath sound was diminished.
Haemogram and peripheral blood smear examination was normal. The erythrocyte sedimentation rate (ESR) was 80 mm in the first hour of examination. Renal and liver functions were normal, as were values for alpha fetoprotein and beta human chorionic gonadotrophin. A tuberculin skin test (Mantoux) was positive, with a diameter of 22 × 20 mm.
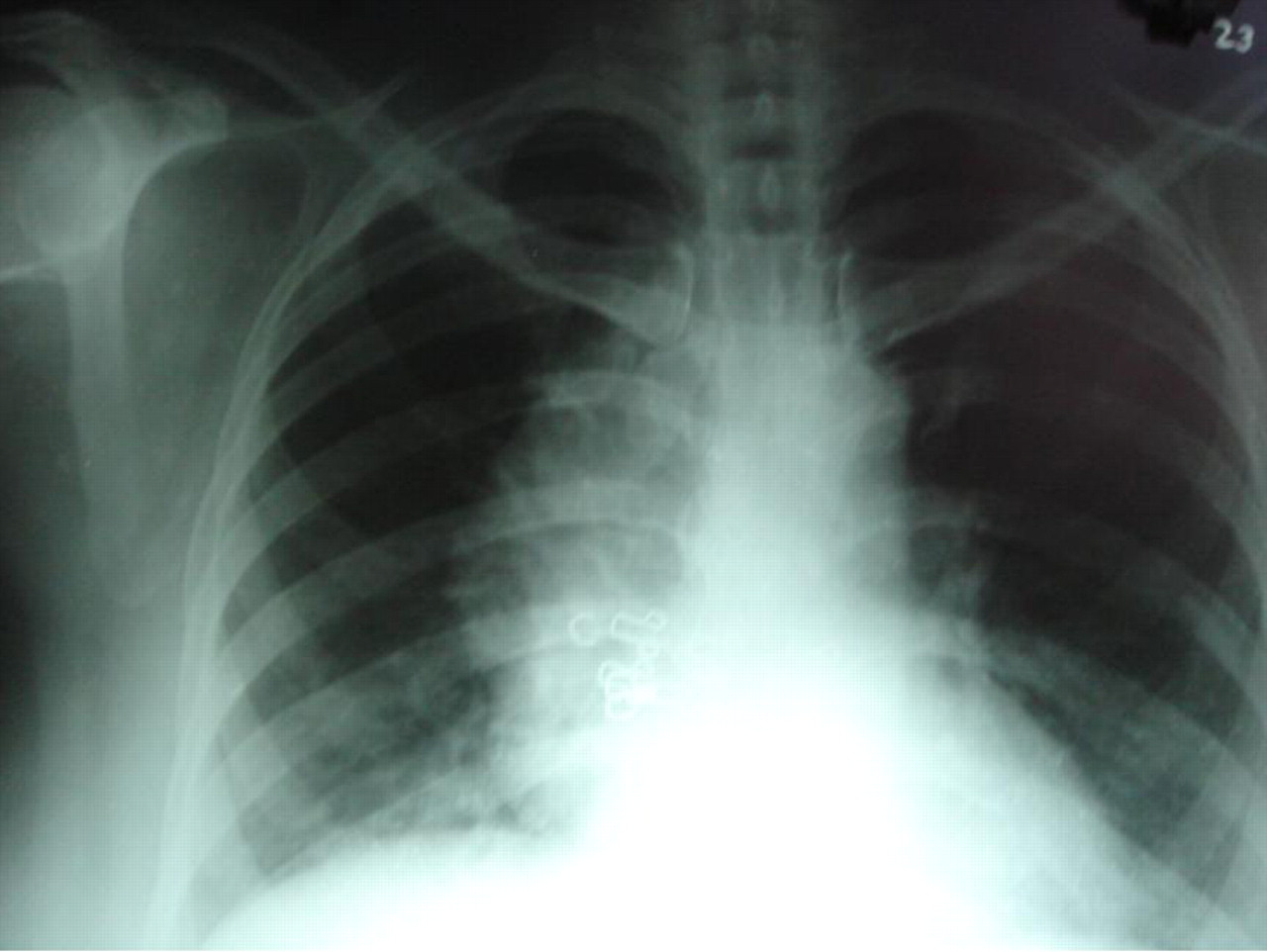
A chest X-ray (postero-anterior view) showed a rounded opacity in the right lung fields arising from mediastinum (Figure 1). Contrast-enhanced computed tomography of the chest showed a large mass arising from the anterior mediastinum. Histopathological examination of the mediastinal mass revealed a chronic granulomatous lesion; however, we were not able to detect any acid-fast bacilli by direct microscopy or by culture. Considering it as a case of tuberculosis, antitubercular drugs (rifampicin, isoniazid, pyrazinamide and ethambutol) were started in the standard dose. The patient showed improvement and a repeat X-ray performed after two months (Figure 2) showed a decrease in size of mass. Anti-tubercular drugs were continued for nine months.

X-ray of the chest showing a large mediastinal mass
X-ray of the chest, two months after starting anti-tubercular treatment, showing a reduction in size of mass
Discussion
The involvement of mediastinum by tuberculosis is an infrequent finding. When it occurs, it is usually in association with parenchymal lesions. The occurrence of isolated mediastinal lymphadenopathy decreases with increasing age 1 and occurs rarely in adults. 2
In an immunocompromised person, the presentation of tuberculosis as a mediastinal mass is not very unusual. 3 But it is rarely suspected in an immunocompetent person when the mass arising from anterior mediastinum is of this size, as in our case. The usual diagnosis of anterior mediastinal masses includes thymoma, lymphoma, teratoma, thyroid masses, vascular tumors, lymphadenopathy due to granulomatous diseases, and so on. In a young person, lymphoma or germ cell tumor is commonly suspected. Diagnosis of germ cell tumor is assisted by the detection of the two tumor markers, viz alpha fetoprotein and beta human chorionic gonadotrophin. But in our case, both were negative.
For the definitive diagnosis of mediastinal tumors, histopathological or cytological examination is a must. In our case, we suspected malignancy as the cause of this mass. But the final diagnosis of tuberculosis was made when we detected a granulomatous lesion in the mass. On histopathological examination, the granulomatous lesion may be due to sacoidosis, tuberculosis or fungal infections. In order to differentiate it, Ziehl-Neelson staining is a quick and definitive method of diagnosis, which is usually not so frequently positive. Culture for Mycobacterium tuberculosis is more sensitive, but it takes a longer time to become positive, causing diagnostic delay. In our case, both culture and staining were negative. But the response to anti-tubercular treatment was very good, thus confirming the diagnosis of tuberculosis.
In the present era when the incidence of tuberculosis is on the rise, it should be regarded as one of the differential diagnoses when clinical and radiological presentation is so atypical.