
Abstract
We conducted a randomized controlled trial comparing EUSOL (Edinburgh University Solution of Lime) and sugar as dressing agents in the treatment of traumatic wounds. Patients in both groups were matched forage and gender. We found EUSOL did better than sugar in terms of contraction of size of wound, presence of discharge, floor area covered with slough, formation of healthy granulation and early possibility of wound coverage.
Introduction
Traumatic wounds are a common cause of morbidity in orthopaedic patients. Therefore, every effort is made to make the wound healthy as early as possible. EUSOL (Edinburgh University Solution of Lime – calcium hypochlorite solution containing <0.25% w/v available chlorine) is a standard dressing material used to remove slough and kill bacteria, an essential process of wound healing. However, it also damages granulation, thus delaying the healing process. 1 EUSOL is an effective antibacterial agent and also assists in slough separation. It appears to be inactive against living tissues and helps obtain healthy granulation tissue. 2
Sugar, due to its hygroscopic nature, makes the slough stick to the dressing gauze promoting removal of slough without damaging the normal tissue. 3 A number of studies have been reported showing results of EUSOL and sugar independently, as case series. A few studies comparing honey to EUSOL have also been reported, proving honey, which acts in a similar manner to sugar, is better than sugar. 4 However, sugar is far cheaper and more readily available than honey. There is no trial comparing EUSOL and sugar in the literature; therefore, the present randomized controlled trial was carried out.
Patients and methods
In 2006, 60 patients presented to B P Koirala Institute of Health Sciences (BPKIHS), Nepal, with traumatic wounds in any part of the limb, and who needed admission and gave informed consent, were selected. We excluded patients with pathological ulcer, loss of sensation, loss of vascularity, cases in which either of the treatments (EUSOL or sugar) was not possible or was contraindicated, and diabetic patients. This left 50 patients available for the study.
The patients were randomly selected for dressing either by EUSOL or sugar. EUSOL was made fresh with 12.5 g of sodium hypochlorite (bleaching powder) and 12.5 g of boric acid in 1 L of lukewarm water and used within 15 min of preparation. For the sugar dressing, commercially available granular sugar was used.
After an initial workup with haemoglobin, random blood sugar and serum protein, all wounds were thoroughly debrided of necrotic and nonviable tissue. The wound was lavaged with normal saline before dressing.
For the EUSOL group, daily dressing was carried out until healing occurred or until granulation tissue appeared. The wound was soaked in EUSOL for 30 min before being packed with EUSOL-soaked gauge. In the sugar group, daily dressing was carried out also until healing or healthy granulation tissue appeared.
The secondary dressing was done by applying sterile gauze pieces and gauze pads in both the groups. Patients were started with oral/intravenous antibiotic empirically followed according to culture and sensitivity of organism grown. The area of the wound was measured in square centimetres by taking an impression of the wound on a gauze piece and tracing it on graph paper on subsequent days. On daily dressing, any unhealthy necrotic tissue which was not responding to either of the dressing material was removed surgically as and when required. The wound area, discharge, area covered with slough and granulation tissue were measured on day 1 and weeks 1, 2, 3 and 4 of follow up.
This study has ethical approval.
Statistical analysis
The data were entered using Microsoft Excel version 8 (Microsoft Corporation, Redmond, Washington). The success of the randomisation was tested by comparing descriptive variables such as age, gender, laboratory parameters and so on. Any discrepancies were measured as the difference between the means in both groups. The significance of these differences was measured using parametric analysis of variance (ANOVA) or the non-parametric Kruskall-Wallis test derived from the Epi Info computer program.
Results
Both groups were comparable in terms of age, gender, lab parameters, and so on (P > 0.05) (Table 1). The wounds in both groups showed improvement with time.
Testing randomization

The mean age of patients enrolled in the EUSOL group was 31.25 years (SD = 16.98) and 32.23 years (SD = 18.27) in the sugar group. In the study by Cannavo et al. 5 the mean age was not similar in three treatment groups (calcium alginate, gauze moistened with 0.05% sodium hypochlorite and combined dressing pad). In our study, male preponderance was seen (78%), which was attributed to more outdoor activities of men compared with women. Students and farmers were more prone to traumatic wounds (40% and 22%, respectively) as they were unguarded and have more outdoor activity. In our study, most patients had associated Gustillo Grade III fractures (62.5% in both the groups), as severity of bony injury is directly related to occurrence and size of wound. Lower limb involvement was the highest in our study (leg – 36%, foot – 14%).
On studying the lab parameters, the mean haemoglobin of patients enrolled in the study was 10.09 ± 2.21 g/dL (EUSOL group = 10.14 ± 2.25 g/dL and sugar group = 10.04 ± 2.23 g/dL) and the mean total serum protein was 6.27 ± 0.88 g/dL (EUSOL group = 6.42 ± 0.88 g/dL, sugar group = 6.13 ± 0.89 g/dL). All the patients were anaemic and were not well-nourished. This corresponds with the study by Gorse & Messner 6 in which the patients were similar for age, blood lymphocyte count, serum albumin and nutritional status.
The patients enrolled in our study had the highest percentage of contaminated wounds (95.83% in the EUSOL group and 88.46% in the sugar group). Injury-debridement interval was 30.7 hours (SD = 56.12) in total, 26.67 hours (SD = 37.3) in the EUSOL group and 34.42 hours (SD = 69.74) in the sugar group. This may be attributed to a lack of good primary care of the wound at district hospitals, poor transport facilities and lack of anaesthesia time in developing countries.
All types of immobilisation were used in our study, but an external fixator was used the most (EUSOL group = 46%, sugar group = 50%).
On an average of two times in hospital, debridement under anaesthesia was carried out in both the groups.
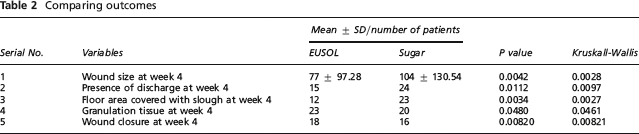
At final follow up at week 4, we could see that EUSOL performed better in terms of contraction of size of wound, presence of discharge, floor area covered with slough, formation of healthy granulation tissue and early possibility of wound coverage (Table 2).
Comparing outcomes
Discussion
Traumatic wounds are a common cause of morbidity in orthopaedic patients. Although their management is considered under plastic surgery, in developing countries where such facilities are not well-developed, an orthopaedic trauma surgeon faces major challenges daily. The associated soft tissue and bony injuries also play a part in the healing of wounds and vice-versa.
The study conducted signifies the importance of the choice of dressing agent that can be used in this setup. EUSOL and other hypochlorites have been used in the past, but questions have always been raised regarding their safety and usefulness. 7 The search for an ideal dressing agent is still ongoing, but seems impossible, as each wound has its own characteristics and therefore requires an appropriate dressing agent. As a result of this, an ideal, safe, cheap and effective dressing agent is yet to be evolved.
The discharge from wounds of patients recruited in our study improved in the EUSOL group on weekly follow ups, but worsened in the sugar group, with the number of patients with purulent discharge increased from 6 (at week 1) to 10 (at week 5). This may be because of uneven distribution of sugar on the wound and of poor slough resorption in the sugar group.
Gorse & Messner 6 compared Hydrocolloid and Dakin's solution and found no significant differences in mean days to healing and decrease in wound area. But we found the floor area covered with slough improved faster with the EUSOL dressing compared with the sugar dressing.
The healthy granulation tissue was found to appear in one case at days 7 and 14 in the EUSOL group when compared with the sugar group. In a study by Subrahmanyam M et al. 8 in 16 patients treated with EUSOL dressing, healthy granulation appeared in week 1 and by week 4 in the remaining patients.
Patients in both groups showed signs of healing with time. However, patients in the EUSOL group showed early signs of healing in the form of granulation tissue formation, epithelisation or keratinisation (healing increased from 17% to 77% at week 4 in the EUSOL group while the increase was only from 12% to 65% in the sugar group).
The probability of healing was also calculated, and was greater in the EUSOL group as compared with the sugar group (EUSOL group = 0.772, sugar group = 0.625). The odds ratio for healing at the end of follow up (week 4) was 1.23, indicating that there is 1.23 times more chance of healing in the EUSOL group as compared with the sugar group. This corresponds with the study by Walker et al. 9 in which they evaluated the effectiveness of EUSOL and sialistic foam dressings in patients admitted with pilonidal sinus or abscess. They found no significant difference in healing time in their study.
This study has shown that EUSOL dressing is better than sugar dressing in terms of improvement in discharge, slough removal, surgical coverage of wound and healing.