
Abstract
Amoebiasis is a common protozoal infection that is endemic in South Asia. Hepatic involvement that manifests as abscess formation occurs in approximately 10% of all patients. Identified expeditiously, this can be treated with metronidazole. We present a case of multiple, large amoebic liver abscesses, that were complicated by thrombus formation in the inferior vena cava extending to the right atrium, requiring surgical removal.
Introduction
Amoebiasis is a common gastrointestinal infection affecting 10% of the world population. 1 It is more common in tropical and subtropical regions and is endemic in south asia. 2 Hepatic involvement is common and may develop in 3–9% of cases, with rates of infection being higher for men. 1,3 Hepatic disease manifests as liver abscess (es), which, if left untreated, may rupture into peritoneal, pleural, pericardial cavities or into bile ducts. 2
Though rare, thrombosis of the hepatic inferior vena cava, referred to as obliterative hepatocavopathy, is a reported complication of hepatic amoebiasis. 2,4,5 However, thrombosis involving the right atrium is extremely rare – only two cases have been reported in the published literature. 4,5 We report a rare case of inferior vena cava thrombus extending to the right atrium in the setting of amoebic liver abscess.
Case history
A 46-year-old man presented to the emergency department with a six-day history of high grade fever, rigors, chills and anorexia. He gave a two-day history of progressively worsening dull abdominal pain, distention and jaundice. He reported normal bowel function. The patient had type II diabetes, well controlled on glimepiride. He had a 20-year history of smoking and was a labourer.
Physical examination revealed a temperature of 38º centigrade, pulse of 108 beats/minute, respiratory rate of 22 breaths/min and blood pressure of 108/77 mmHg. His oxygen saturation at room air was 97%. He was moderately dehydrated and icteric. His abdomen was moderately distended, soft and tender in the right hypochondrium. There was no evidence of peritonitis. The liver was palpable 4 cm below the costal margin. Bowel sounds were present and a digital rectal examination was unremarkable. The remaining examination was unremarkable.
Initial laboratory investigations revealed haemoconcentration, marked leucocytosis (predominantly neutrophilia with a left shift), mild liver function dysfunction and a deranged prothrombin time. Detailed values are listed in Table 1.
Results of laboratory investigations
An ultrasound examination of the abdomen revealed two subtle heterogeneous areas in the right lobe of the liver. The larger area measured 6.6x5.5 cm and was posterior to the main portal vein. The second area measured 5.4x3.8 cm within the superior segment of the right lobe. Bilateral polycystic kidneys were also noted. An indirect haemagglutination assay (IHA) for entamoeba histolytica was positive (1:512).
The patient was resuscitated and treatment with metronidazole 750 mg every eight hours was initiated. Over the next 48 hours there was a significant improvement in the symptoms, with an improvement in pain scores. He remained afebrile. However, on the third day of admission, he became short of breath and complained of worsening right upper quadrant pain. A chest X-ray revealed bilateral pleural effusion and right base atelectasis. Arterial blood gases revealed hypoxia and hypocarbia (oxygen pressure 76 mmHg, carbon dioxide pressure 26 mmHg). A computerized tomography scan of the abdomen showed two large abscesses in the liver. One was located in segment IV and measured 7x6 cm and the other lying adjacent to the capsule in segment V measured 8x5.7 cm (Figure 1A). No evidence of abscess rupture was seen. However, the inferior vena cava (IVC) was externally compressed by one of the abscesses and a low attenuation thrombus-like lesion was discovered which partially occluding the lumen (Figure 1B) and extended into the cavity of the right atrium (Figure 1C). Under ultrasound guidance, the larger abscess was aspirated and 20 mL of thick pus was removed. A 19-French pigtail catheter was placed in the cavity. There were no trophozoites seen on the microscopic evaluation of the pus and no organisms were isolated on culture. A coagulation workup was done including proteins C and S, Factor V-Leiden and antithrombin III that showed non-specific derangement, probably associated with inflammation (Table 1).
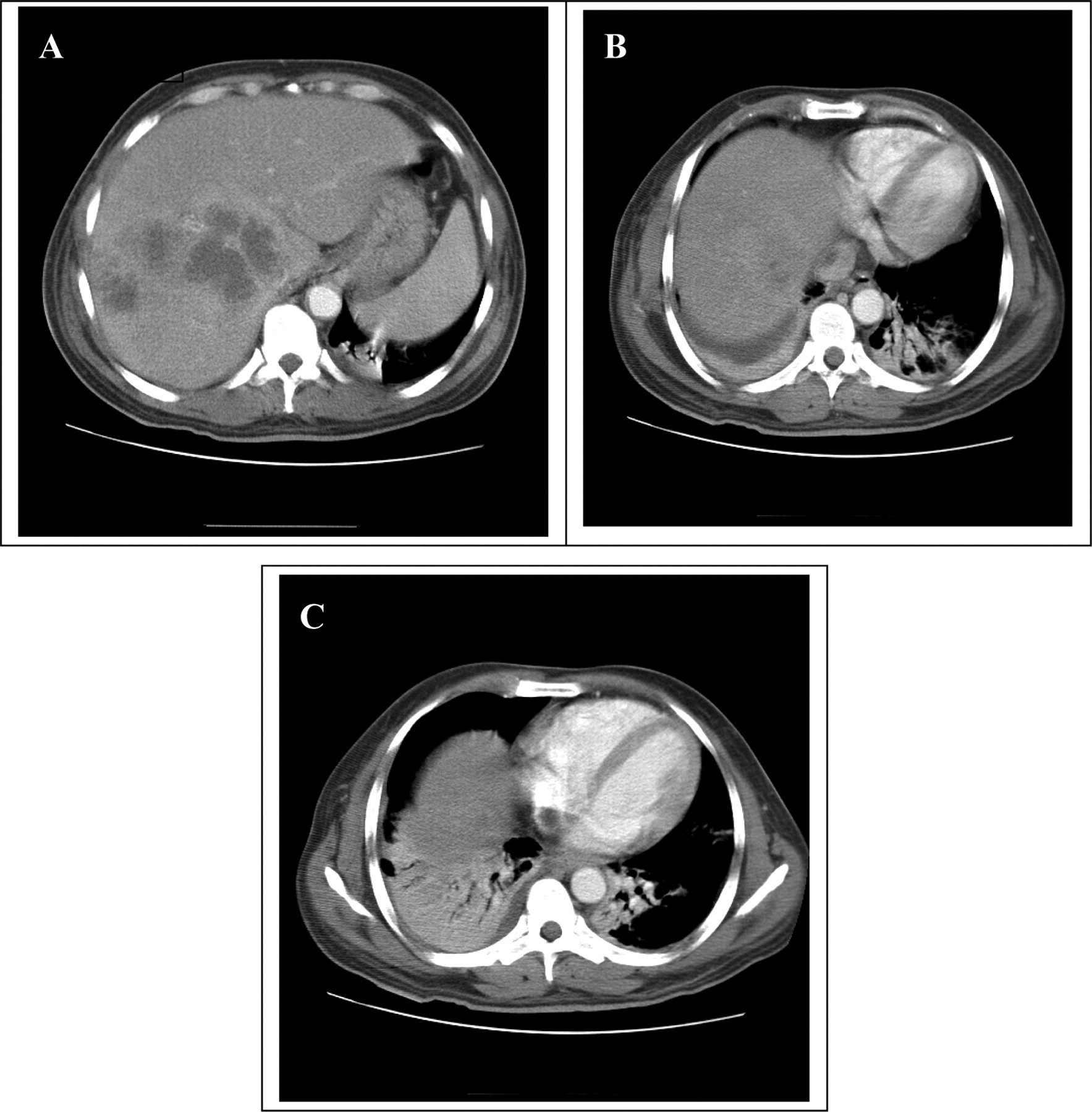
(A) Multiple abscesses in the right lobe of the liver and an almost collapsed inferior vena cava (IVC) in the vicinity of an abscess; (B) thrombus in the IVC; (C) thrombus reaching the right atrium
A two-dimensional echocardiogram identified an echogenic mass extending from the IVC to the right atrium which was freely mobile and was deemed to have potential for detachment and embolization.
The patient was heparinized and an emergent medial sternotomy and right atriotomy was done. A yellowish-grey mobile thrombus, measuring 4x1.5x0.5 cm, extending superiorly from the IVC, was removed. Microscopic examination confirmed it to be a thrombus. Postoperatively, the patient was anticoagulated with low molecular weight heparin, followed by warfarin. He made an unremarkable recovery and was discharged on the seventh post-operative day. He was being followed in outpatient clinics. His international normalized ratio was maintained at between 2.5 and 3. He remained well with resolution of the abscess cavities and no evidence of vascular abnormalities in the liver.
Discussion
Amoebic infection is common in the developing world with amoebiasis being second only to malaria as parasitic cause of death. 2,3 Entamoeba histolytica is the most frequent pathogen that gains access to the gut by the oro-fecal route. The invasive trophozoite, invades the mucosa causing amoebic colitis. The mucosal barrier may be breached, allowing access to the liver via the portal circulation. Here liquifactive necrosis occurs, forming the abscess which is comprised of dead and dying hepatocytes, manifesting as the characteristic ‘anchovy paste’ pus. In the past, these abscesses have often proved fatal. However, nowadays they can be managed easily with the amoebicidal metronidazole. These abscesses may be complicated by rupture. Thrombosis of the IVC is a rare complication. 2,4,5 Some cases of Budd-Chiari syndrome have also been reported in association with amoebic liver abscesses. 6 However, thrombus extention into the right atrial cavity is an extremely rare complication related to amoebic liver abscess with only two cases reported in literature thus far. 4,5
The exact pathophysiology of IVC thrombosis occurrence in hepatic amoebiasis is uncertain. Proposed mechanisms include external mechanical compression, thrombotic state associated with the inflammatory process of amoebiasis, an adjacent spread of inflammation, diaphragmatic movement and coughing. 2,6,7 External compression causes anatomic distortion of the vein which, in turn, alters the flow dynamics favouring turbulence and stasis of blood which may lead to thrombosis. Inflammatory processes associated with the amoebic abscesses could potentially predispose a patient to a thrombotic state. Derangement of coagulation factors such as that seen in our case (Table 1) has been described by Okuda. 7 In cases of hepatic abscess in close proximity of the IVC, the inflammatory process in the wall of the abscess may spread and cause injury to the wall, leading to inflammation followed by thrombosis. 2 Respiratory movements of the diaphragm and coughing might cause injury to the IVC endothelium predisposing a patient to IVC thrombosis. 7 The thrombotic state may be compounded by dehydration due to poor oral intake in a patient with amoebiasis.
In our case we suspect that external mechanical compression due to multiple large abscesses was the primary cause of thrombus formation. The concurrent inflammatory process with associated thrombotic coagulation profile and dehydration as probably acted as precipitating factors for thrombus formation.
Ultrasound of abdomen should be considered in patients with fever and abdominal pain for more than seven days, especially in endemic areas. 2 We suggest that the hepatic abscess (es) in close proximity to the IVC or hepatic veins or ≥5 cm in size, should be investigated for any evidence of distorted IVC anatomy using CT or Doppler ultrasonography. Coagulation system should be assessed in order to rule out a thrombogenic state, although the significance of these abnormalities is uncertain in the setting of acute infection/inflammation.
Any patient who does not respond as expected to standard medical therapy should be investigated further in order to detect complications. Decompression of the lesion(s) should be considered if an anatomical distortion of the IVC or hepatic veins is identified as this can help to reduce the risk of thrombosis. 6
Anticoagulation therapy and subsequent warfarization is the standard treatment of venous thrombosis while thrombolysis is evolving as a new trend and has been used successfully in a case of IVC thrombosis secondary to hepatic amoebiasis. 5 No reported case of right atrium thrombosis in association with amebic liver abscess needed surgical intervention. In our patient, a partially occluding thrombus with a free floating end in right atrium and flow in the IVC could be expected to have a greater risk of dislodgement and subsequent pulmonary embolism. We felt that this finding merited emergency surgical intervention.
To conclude, we believe that this is the first such case reported of a potentially lethal complication of amoebic liver abscess. Based on a high index of suspicion, because of incomplete response to standard treatment, the patient was thoroughly investigated with ultrasound, a computerized tomography scan and an echocardiography and the potential disaster was averted with timely surgical intervention.