
Abstract
Dirofilariasis is a common filarial infection occurring in domestic and wild animals as a result of arthropod bites. However, it can be transmitted to humans after mosquito bites. Here, we report a case of a 54-year-old lady who developed an unilateral eyelid swelling secondary to Dirofilaria repens.
Case history
A 54-year-old woman presented with complaints of a swelling of the right eye associated with mild itching of six weeks' duration. The swelling was of sudden onset and progressed slowly leading to an inability to open the eye. There was no associated pain or redness. Before presenting to the dermatology outpatients department of the Kasturba Medical College, Manipal, she showed a mild symptomatic improvement following four injections of corticosteroids prescribed by a local doctor. She was a known diabetic and had been on medication for two years.
Local examination revealed a diffuse non-tender swelling of the right upper eyelid with a diffuse cord-like induration beneath the skin just below the eyebrow. The cord-like structure extended medially for about 2 cm starting from just above the lateral canthus. The overlying skin was shiny, oedematous and mildly hyperpigmented (Figure 1).

Diffuse swelling of the upper eyelid
The ocular movements, anterior segment and fundus, of both eyes were normal. The blood picture was normal with an absolute eosinophil count of 300 cells/mn. A stool examination using the concentration technique did not show any ova or cysts. A computerized tomography scan showed soft tissue swelling of the right upper eyelid without any calcification. The right globe, including optic nerve and the extra ocular muscles, were normal with no proptosis. An excisional biopsy from the swelling revealed cross sections of degenerating filaria with a thick laminated cuticle, distinct longitudinal ridges and an intense surrounding inflammatory reaction of lymphocytes, plasma cells, histiocytes, eosinophils and giant cells (Figure 2).
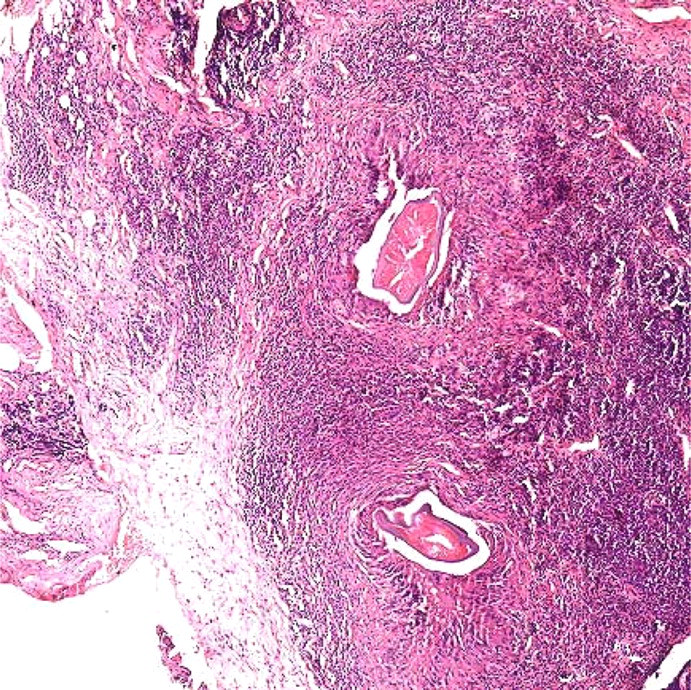
H&E slide showing cross sections of larvae and dense inflammatory infiltrate in the dermis
A possibility of dirofilariasis was considered and the patient was referred to the plastic surgery department for exploration and complete excision of the cord. Surgical exploration by transverse incision over the cord-like structure revealed thickened skin (thickness varying from 1–2 mm) with a whitish firm and fibrous structure approximately 2 cm long just below and adherent to the dermis but not fixed to the underlying muscle. The subcutaneous tissue was also thickened (approximately 3 mm) but the underlying muscle appeared to be normal.
The surgically excised samples of skin, cord-like structure and subcutaneous tissue were sent to the Centres of Disease Control, Atlanta, USA. The diagnosis of dirofilariasis was confirmed: the worm, probably a young worm, was a Dirofilaria repens. The overall diameter of the worm was 206 µm. The multilayered cuticle ranged in thickness from 8.8 µm to 15.4 µm. The flattened dome-shaped cuticular ridges ranged from 6–8 µm apart in thicknesses ranging from 8.8 µm to 15.4 µm (Figure 3). The sex could not be established due to the degradation of the internal morphology. The patient was prescribed diethylcarbamazine for four weeks. Seven months after surgical excision a mild swelling of the eyelid persisted.
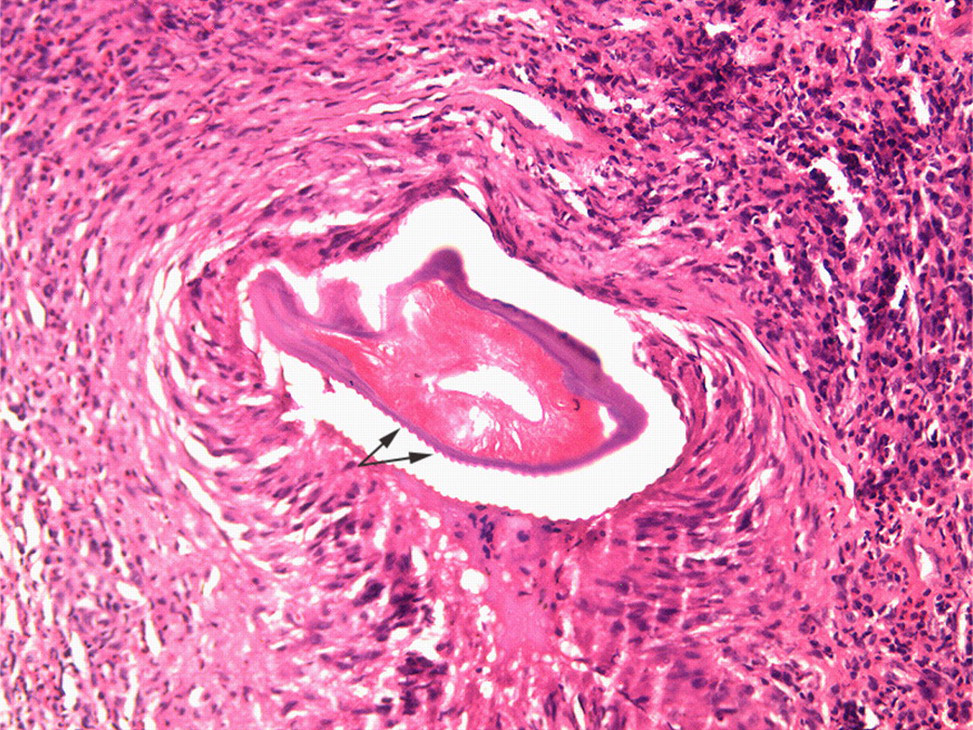
The characteristic cuticular ridges of Dirofilaria repens
Discussion
Dirofilariasis is a common filarial infection usually occurring in domestic and wild animals which are infected after arthropod bites. The microfilariae in the blood stream can be transmitted to other animals. Transmission to humans occurs after a mosquito bite. As man is an unnatural host, the microfilariae cannot mature fully and microfilaraemia is uncommon. 1
Dirofilariasis usually presents as subcutaneous nodules or ocular lesions. There may be localized itching and a crawling sensation under the skin. Rarely, allergic reactions of fever, urticaria and facial oedema may occur. The subcutaneous tissues, the eyelids and the periorbital region are common sites of involvement of ocular adnexa but subconjuctival involvement is rare. 2 Subcutaneous dirofilariasis is exclusively due to D. repens in Asia. 1
Treatment of dirofilariasis is by surgical excision of the lesions with or without chemotherapeutic drugs such as diethylcarbamazine or ivermectin. The cure can be confirmed serologically by estimating the levels of immunoglobulin G antibodies in the serum by immunoenzymatic assays which show a progressive decline which ultimately becomes negative after six months of surgical extraction. 3
Our patient was from Kerala, a south Indian state where about 7% of the dogs have tested positive to microfilariae of D. repens. 4 The clinical diagnosis of dirofilariasis is difficult except in instances where a protruding worm can been seen. 5 In our case the clue to a parasitic disease was the mild itching at the onset of the swelling and the cord-like structure palpable in the subcutaneous tissue. The patient was treated with diethylcarbamazine for four weeks. At the seven months follow-up her only symptom was mild persistent oedema possibly as a side effect of the surgery.