
Abstract
Acanthosis nigricans (AN) is a dermatological condition that is often associated with obesity and may be a physical marker of insulin resistance. Studies have documented a high prevalence rate of AN in people with diabetes mellitus (DM). However, there have been no Nigerian reports on AN and DM. This report bridges the information gap and documents the prevalence of AN in Nigerians with type 2 DM as well as its clinical correlates. Three hundred and forty consecutive subjects with type 2 DM were examined for the presence of AN and its associated clinical features. The prevalence of AN in type 2 DM in this report is 17%. Factors associated with AN include obesity, a family history of DM, female gender, the presence of hypertension and poor glycaemic control.
Introduction
The prevalent form of diabetes mellitus (DM) is type 2 DM which is characterized by hyperinsulinaemia and/or insulin resistance, either of which may be the predominant feature. 1 Acanthosis nigricans (AN), a skin condition frequently associated with insulin resistance and obesity, may be present in people with type 2 DM. 1–2 There are many reports which confirm that AN is more common in black people and African-Americans than in caucasians in which the prevalence rates range from 41–74%. 1–3 However, there is a dearth of reports on AN from sub-Saharan Africa.
Methods
Three hundred and forty consecutive patients with type 2 DM were recruited from the DM clinic of the Department of Medicine of the Lagos State University Teaching Hospital, Ikeja, Nigeria. The exclusion criteria included pregnancy, women who had used oral contraceptive agents and those with a documented malignancy. The body mass indices (BMI) and waist circumferences were documented. Central obesity was said to be present for men with a waist circumferences of ≥94 cm and women with a waist circumferences of ≥80 cm. 4 The flexures of the neck were examined for the presence of AN.
Discussion
In our study the prevalence rate of acanthosis nigricans was 17% which is much lower than in other reports. 5–6 There was a noted female preponderance of DM subjects with AN with a documented female:male ratio of 3:1. Table 1 shows the biodata, demographics and anthropometric indices of the study subjects. The prevalence of obesity was 69%. A higher proportion of subjects with AN had centripetal obesity. Although we found an association of AN with obesity, its occurrence is not necessarily associated with increasing BMI levels (Figure 1). The association of acanthosis nigricans with high anthropometric indices in those with type 2 DM may be likely pointers to one of the underlying pathophysiological mechanisms of type 2 DM which is insulin resistance. AN, though more common in the obese, can however occur in those of normal weight or, albeit uncommonly, in underweight people. In this study, subjects who were underweight and of normal BMI accounted for 20% of those with acanthosis nigricans.
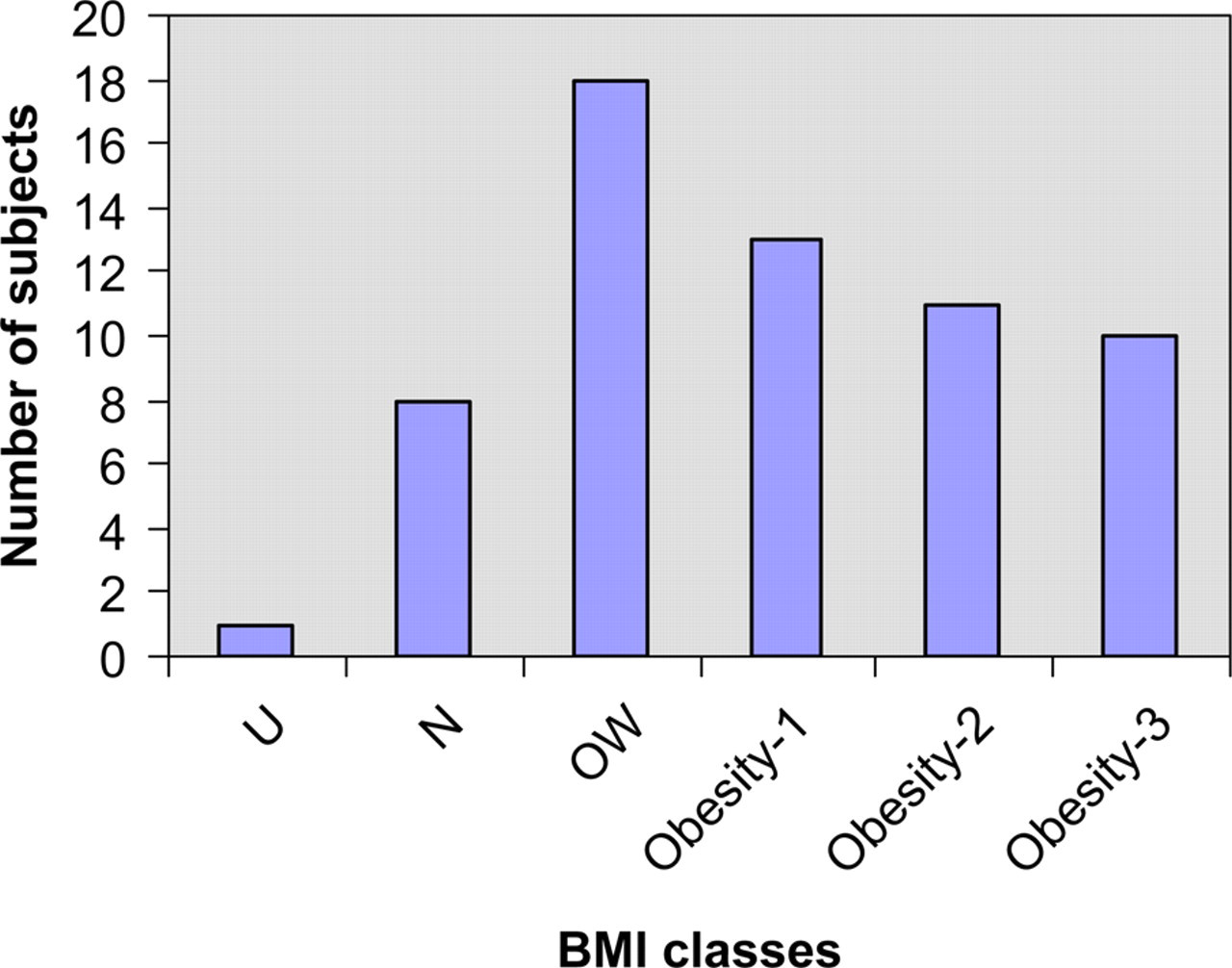
Distribution of diabetes mellitus subjects with acanthosis nigricans by body mass index. U, underweight; N, normal weight; OW, overweight; obesity-1, class 1 obesity; obesity-2, class 2 obesity; obesity-3, class 3 obesity
Biodata, anthropometric indices and demographic data of study subjects
AN, acanthosis nigricans; BMI, body mass index; WC, waist circumference; F, female; M, male
A family history of DM and the presence of hypertension were notable features of DM patients with AN. Kong et al. 6 reported that children and adults with a family history of type 2 DM had more than twice the prevalence of AN. Hypertension, an often reported comorbidity of DM, which has been implicated as a determinant of DM hospitalization outcome in Nigeria, 7 was noted in 66% with a female: male ratio of 2:1.
The documented mean fasting plasma glucose in this study, though generally in the poor glycaemic control range, was found to be higher in subjects with AN and this difference was statistically significant. Less than a third (36; 11%) used insulin and of those 19 (53%) were on a combination of oral hypoglycaemic agents and insulin. Daily insulin dosages used ranged from 14–60 IU daily. There was a female preponderance of DM subjects with AN.
Conclusion
A significant proportion of DM subjects with AN had a first degree family history of DM. Despite the low incidence of AN in DM, we suggest that its presence in association with a family history of DM may be useful as strong indicators for screening for DM especially in resource-limited economies. Optimal treatment of Nigerians with type 2 DM may necessitate the usage of insulin either solely or in combination with oral insulin sensitizing agents.