
Abstract
Hydatid disease is an endemic parasitic disease prevalent in sheep-rearing countries. Although liver and lung are the commonly involved organs, hydatid disease can occur in any organ or tissue. In this case series, we share our experience of some rare primary extrahepatic intra-abdominal hydatid cysts.
Introduction
Hydatid disease (HD) is caused by the larval stage of Echinococcus granulosus. It is a significant health problem in underdeveloped areas where animal husbandry is common but where no veterinary control exists. E. granulosus can reach any organ or tissue in the body where it then develops into small hydatid cysts. Clinical, radiological and serological tests may be helpful in the diagnosis, but their reliability is not 100%. Man is an accidental intermediate host. As such, unusual sites (10–15%) may cause diagnostic problems that might lead to an increased risk and potentially serious complications, even mortality (4%). The purpose of this report is to emphasize the fact that HD should be suspected when there are cystic lesion affecting any organ in the body, especially in endemic areas of the world. We describe some unusual sites of this disease.
Case history
Case one
A 35-year-old Indian woman presented with a four-month history of pain in the upper abdomen and a yellowish discoloration of the urine. The physical examination revealed jaundice. The abdominal examination was normal. The haematological examination revealed mild pallor (9 mg %) with marked eosinophilia (17%) and a raised erythrocyte sedimentation rate. The liver function test was consistent with conjugated hyperbilirubinaemia (total bilirubin-13.8 mg%, direct bilirubin-10 mg%, alkaline phosphatase-2254 U/L, alanine aminotransferase-113 IU/L [reference range 0–50 IU], aspartate aminotransferase-152 IU/L [reference range 6–40 IU]). Computerized tomography (CT) of the abdomen reported a well-defined cystic space occupying lesion (SOL; 52 × 40 mm) at the neck of the pancreas (Figure 1) with no evidence of mural nodularity, internal solid component or septa. The main pancreatic duct was dilated. The common bile duct (CBD) was compressed at its lower end by the cystic SOL at the pancreatic neck. A radiological diagnosis of mucinous cystic neoplasm or pseudocyst of pancreas was made. Magnetic resonance computerized pancreatography revealed a necrotic mitotic pancreatic mass. Pancreatic tumour markers for pancreatic neoplasm carcinoembryonic antigen (1.1 ng/mL, n = 0–3.4 ng/mL), CA 125 (7.5 U/mL, n = 0–35 U/mL), CA 19–9 (2 U/mL, n = 0–37 U/mL) were done and found to be within normal limits. An enzyme-linked immunosorbent assay (ELISA) for hydatid was strongly positive. At laparotomy a cystic mass was found bulging from the head of the pancreas. The cyst was aspirated and opened. A collapsed germinative membrane was found and removed. There was a residual cavity that had no communication with the pancreatic duct. The content of the cyst was removed without any spillage and a cystogastrostomy was performed. Postoperatively, albendazole was prescribed (800 mg/day). The patient was started on 800 mg/day albendazole after surgery. Recovery was uneventful and follow-up asymptomatic. The patient has remained symptom-free. Hydatidosis was confirmed histopathologically.
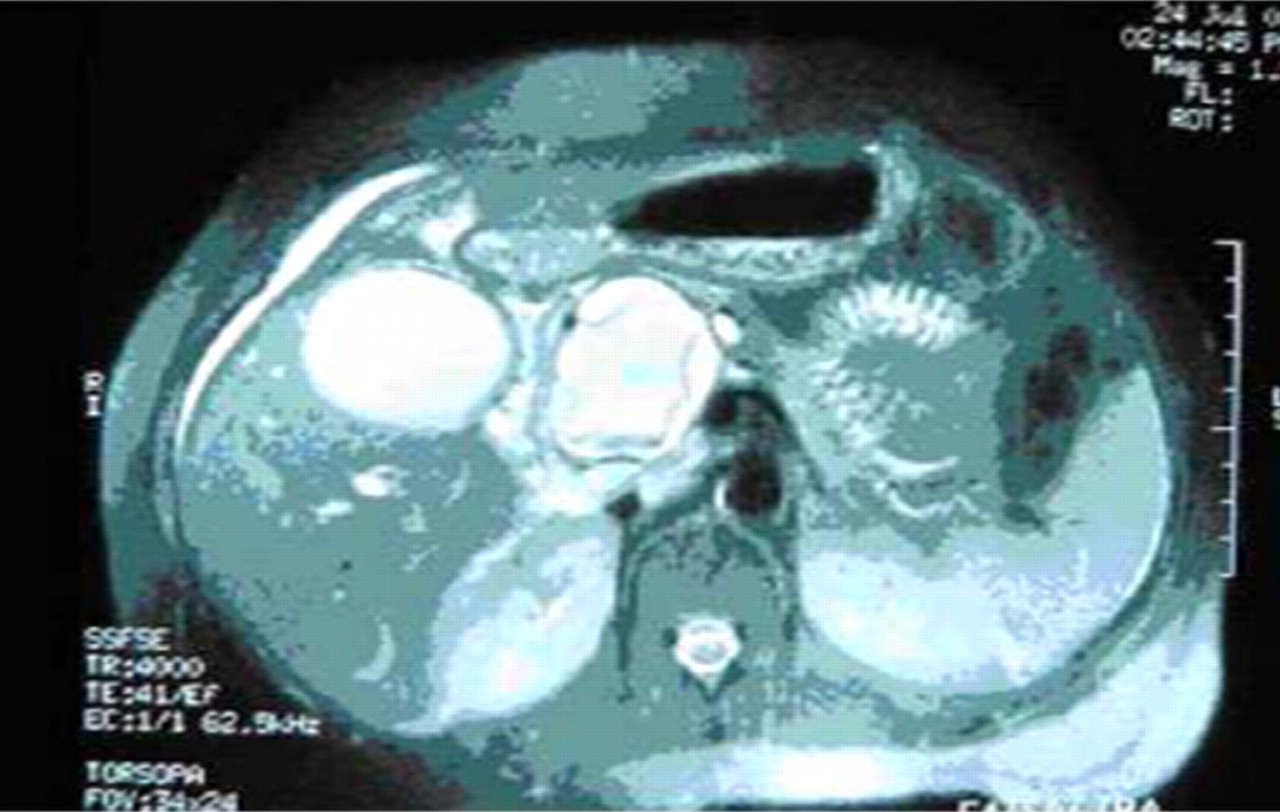
A computerized tomography scan showing a hydatid cyst in the pancreatic head
Case two
An 11-year-old girl presented with pain in her upper abdomen, an abdominal mass and a five-month history of jaundice. Clinical examination revealed icterus, a solitary mobile mass measuring 8 × 6 cm in the right upper quadrant. The laboratory investigation was consistent with conjugated hyperbilirubinaemia (total bilirubin-6.4 mg/dL, direct bilirubin-3.5 mg/dL) with raised alkaline phosphatase. Other parameters were within the normal limits. Abdominal ultrasonography (USG) and CT were consistent with a type 1 choledochal cyst (Figure 2). An operation revealed that the gall bladder was edematous and distended. The common bile duct (CBD) was replaced by a fusiform swelling measuring 9 cm × 8 cm × 8 cm (Figure 2). Palpation of the gall bladder revealed no stones. Cholecytectomy was performed and a progressive dissection of the CBD for Roux-en-Y hepaticojejunostomy was undertaken. The tapered lower end of the retroduodenal CBD was dissected, transected and ligated. The proximal section of the CBD was dissected up to about 1 cm below the hilum. On transection of the proximal part of the dilated duct, the choledochotomy revealed an unruptured solitary cyst with a germinative membrane, and a diagnosis of a hypertrophic cardiomyopathy (HC) was made. A cholecystectomy and Roux-en-Y hepaticojejunostomy was performed. Hydatidosis was confirmed histopathologically. The patient made an uneventful recovery. The patient was discharged on the twelfth postoperative day with a 20 mg/kg/day dose of albendazole and was still doing well after two years.

A postoperative specimen showing the gall bladder, excised common bile duct and the hydatid cyst
Case three
A 24-year-old man presented with a 12-year history of a painless lump in the left upper abdomen. The physical examination was normal. Examination of the abdomen revealed a splenic swelling which gradually increased in size. An USG (ultrasonography) of the abdomen revealed a splenic (14.6 cm × 8.6 cm) cystic SOL with an internal cystic loculi, echogenic foci and a tongue-like projection in the inferomedial aspect of the spleen consistent with HD. A CT scan of the abdomen confirmed the USG findings. An enzyme-linked immunoadsorbent assay (ELISA) for hydatid was positive. A splenectomy was performed and the specimen was cut open to display the HC. The patient was discharged on the tenth postoperative day after the stitches had been removed and was given a course of albendazole (800 mg/day). The patient was well after six months of follow-up.
Case four
A 56-year-old woman presented to the emergency department with acute right lower abdominal pain, nausea and vomiting associated with fever. She was thin and her vital signs were: pulse of 110/min; blood pressure 110/70 mmHg; respiratory rate 26/min; and a 39°C temperature. An abdominal examination revealed a tender firm mass in the right iliac fossa, measuring 5 cm × 3 cm, with restricted mobility. Muscle guarding was present over the lump. Straight leg rising, cough sign and rebound tenderness was positive. Other areas of the abdomen did not reveal any significant abnormality except for mild abdominal distention. Further investigations were conducted to address a clinical suspicion of an appendicular lump.
Laboratory investigations revealed a haemoglobin level of 9.2 g/dL, neutrophilic leucocytosis (16,000/mm3) and marked eosinophilia (19%). USG of the abdomen revealed a multiseptated cyst (5.2 cm × 2.5 cm) with a honeycombed appearance in the right iliac fossa, suggestive of HC.
At laparotomy the cyst was found to be located in the appendicular mesentery, bordered by the appendix, terminal ileum and caecum. An enucleation of the HC was performed. There were no cysts in any other areas of the abdomen. The patient made an uneventful recovery with a return to a normal appetite. She was discharged on the tenth postoperative day with a prescription for albendazole 400 mg twice a day. She was kept under regular follow-up and there has been no recurrence of the HD.
Discussion
HD is endemic in cattle- and sheep-raising regions such as India, Central Europe, the Mediterranean countries, the Middle East, South America, Australia, New Zealand and South Africa. 1–11 Dogs or other carnivores are definitive hosts of HC, whereas sheep or other ruminants are intermediate hosts. 4,7,8 Humans are secondarily infected by the ingestion of food or water that has been contaminated by dog faeces containing the eggs of the parasite. 1,6,7,9 After the outer capsule of the egg has been ingested, the freed embryo (oncosphere) enters a branch of the portal vein by passing through the duodenal mucosa. Most of these embryos become lodged in the hepatic capillaries, where they either die or to grow into HC. 2,4–7 Some pass through the capillary sieve and become lodged in the lungs and other organs. There have been reports of lymphatic spread. 6,7,8
The most common sites include the liver (59 75%), lungs (27%), kidneys (3%), bones (1 4%) and brain (1 2%). 1,2,3,9–11 The peritoneal cavity (primarily or secondarily), pancreas, common bile duct, spleen, heart and muscles are rarely affected. 8–11 Peritoneal HC, either primary or secondary, represents an uncommon but significant (13%) manifestation of this disease. 2,4 It is always secondary to the traumatic or surgical rupture of a hepatic splenic cyst. 2,3,10 CT is the modality of choice for these patients because it permits the imaging of the entire abdomen and pelvis. 3 The lesions are generally multiple and can arise anywhere in the peritoneal cavity. Unilocular cysts should be distinguished from mesenteric cysts or intestinal duplication cysts. 2,6,10
Primary splenic involvement is very rare (0–2%).The symptoms are mainly abdominal pain, splenomegaly and fever. Splenic HCs are usually solitary and their imaging characteristics are similar to those of hepatic HCs. 2,10 Other splenic cystic lesions such as splenic HC should be considered in the differential diagnosis but should be differentiated from epidermoid cyst, pseudocyst, splenic abscess, haematoma and cystic neoplasm of the spleen. 10
Primary HC of the pancreas is rare (0.2–2%). It is usually single and located in the head of the pancreas. 2,3,9–11 The clinical symptoms depend on the size and location of the cyst within the pancreas. The lesion in the head of pancreas frequently presents with jaundice due to the obstruction of the common bile duct. However, the body or tail lesions rarely cause symptoms. The differential diagnosis includes abscess or cystic neoplasms of the pancreas. 10,11 The typical appearance and location of HCs within the pancreas has not been established due to their relatively rare occurrence. 2
The association of HC and jaundice is unusual (5–17%). 7–9 An intrahepatic HC causing obstruction and compression of the intrahepatic biliary ducts, resulting in jaundice, is the most common form seen. 8,9,10 Extrahepatic biliary obstruction by a HC is rare and is usually caused by the rupture of the hepatic cysts into the biliary tract with resultant obstruction by the contents of the cysts. Extrahepatic biliary obstruction by HC without hepatic involvement is the rarest presentation. 10 A solitary extrahepatic choledochal HC without any hepatic involvement, causing an intrinsic obstruction of the CBD, is unknown.
The clinical presentation of HD depends on the size and site of the lesion and the accessibility for clinical examination of the organ involved. Pre-operative diagnosis of HC can be made and confirmed by CT, MRI and USG 2–4 Serological tests (immunoelectrophoresis, ELISA, latex agglutination and indirect haemagglutination test) are complimentary to radioimaging for the diagnosis, screening, postoperative follow-up and relapses after surgery. 5–7
Surgery is the treatment of choice for large HC. 5–11 Uultrasound-guided percutaneous aspiration of cysts followed by injection of protoscolicidal substances and re-aspiration is another mode of treatment indicated for: large, multiple cysts of the liver, spleen, kidney and bones; inoperable cases; and relapses after surgery. The contraindications are lung cysts and communicating cysts. 7–11
Albendazole should be given both preoperatively and postoperatively. 7 The dose duration is five days before, to one month after, the operation. A 40% success rate for such cases has been reported. 7,8 Antihelminthics work best when prescribed for small, unilocular HC. Antihelminthics sterilize the cyst, decrease the chance of anaphylaxis, decrease the tension in the cyst wall (thus reducing the risk of spillage during surgery) and reduce the recurrence rate postoperatively.
The recurrence rate of hydatid disease after surgical treatment is approximately 2%. 8 The survival rate for patients undergoing operative intervention is 95%. 6,7 A postoperative long-term follow up with imaging every six weeks is essential. 7
We conclude that E. granulosus can affect any organ in the body and a high suspicion of this disease is justified in any cystic neoplasm of any organ, especially in endemic regions. Moreover, medical treatment should precede and follow the surgical intervention.