
Abstract
The primigravid uterus is believed to be immune to rupture during labour. This may not be true for those who have had prior adenomyomectomy, hence this report. The patient was a 28-year-old nullipara who became pregnant 11 months after an adenomyomectomy. Twelve hours after vaginal delivery at term, she developed haemoperitoneum of unclear cause. Emergency laparotomy and subsequent histology showed a fundal complete uterine rupture through the adenomyomectomy site, which was repaired. It is concluded that adenomyomectomy predisposes a pregnant uterus to rupture during labour. Therefore, such women should be offered elective caesarean delivery at term.
Case history
The patient was a 28-year-old nullipara. As part of her management for infertility of two years' duration, she had elective laparotomy and adenomyomectomy of a fundally located adenomyoma on 28 February 2006 at a teaching hospital in Nigeria. The endometrium was not breached during the surgery. She became pregnant 11 months after the surgery with a last menstrual period on 12 February 2007. The pregnancy was uneventful and she received antenatal care at the same hospital. Her packed cell volume (PCV) at 37 weeks' gestation was 34%. She had a vaginal delivery of a live boy who weighed 3.4 kg at a gestational age of 38 weeks plus two days. The labour was neither induced nor augmented. Her one hour post-partum vital signs were normal and she was transferred to the post-natal ward.
About 12 hours after delivery, she complained of progressive weakness, abdominal distension and dizziness on sitting-up from a lying-down position. On examination, she was conscious, alert but severely pale. Her pulse was 112 beats per minute, of small volume and regular. Her blood pressure was 90/50 mmHg. The chest was clear on auscultation. There was tarchycardia but no murmur. The abdomen was grossly distended with marked suprapubic tenderness (Figure 1). The uterus was of about 18 weeks' gestational size. The abdominal gait was 87 cm and measured 14 cm inferior to the xiphysternum. The fluid thrill was equivocal. There was no active vaginal bleeding. A diagnosis of post-partum hypotension due to haemoperitoneum of unclear cause was made. An urgent PCV was 20%. Resuscitation was commenced with intravenous crystalloids. A unit of whole blood was given. An urgent abdomino-pelvic ultrasound showed massive haemoperitoneum.
Distended abdomen of the patient prior to surgery
Emergency laparotomy showed a haemoperitoneum of about 2.5 L and an oval area of complete fundal uterine rupture of about 4 × 3 cm in diameter. The defect was plugged by friable haemorrhagic tissue surrounded by yellowish adenomyomatous tissues. As much as possible of these were excised (Figure 2). The uterus was repaired in two layers with two chromic catgut sutures and two extra units of blood were transfused. She made a quick recovery and her post-operative PCV was 28%. She was counselled on elective caesarean delivery at 36 weeks' gestation in subsequent pregnancies. She was discharged home on haematinics on the eighth day post-partum. The histology of the surgical specimen showed adenomyosis.
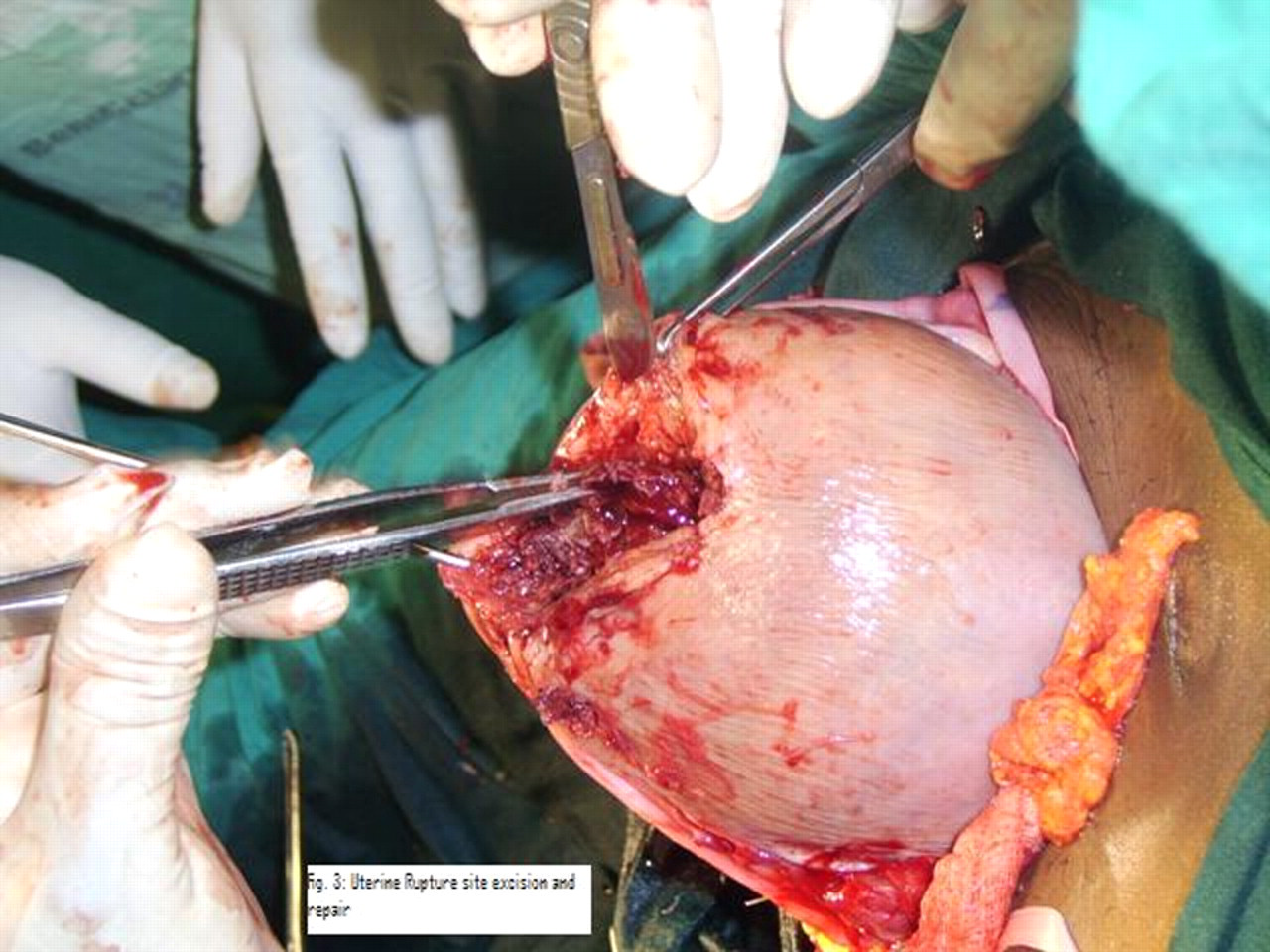
Uterine rupture site excision and repair
Discussion
Adenomyosis is the presence of endometrial gland and stroma within the uterine musculature. 1 The aetiology of adenomyosis in our patient is not known. During the elective laparotomy, the conservation of the uterus was very important considering her age. Otherwise, abdominal hysterectomy would be the treatment of choice for adenomyosis. 1 Myometrial excision (adenomyomectomy) produces uterine scar(s) which may contain foci of undetectable adenomyosis with reduced tensile strength which thereby increases the risk of uterine rupture during pregnancy. 2 This may explain the development of an area of low uterine wall resistance in our patient which ruptured during labour.
Although adenomyosis may not be uncommon in Nigeria, 3 a literature search did not reveal any similar reports. The preponderance of the condition in multiparous women 3 who might have completed their reproductive functions may explain this rarity. However, antenatal and intrapartum uterine rupture after adenomyomectomy have been reported from other parts of the world. 4,5
There was no doubt that the patient would opt for supervised antenatal care and elective cesearean deilvery for future pregnancies and so the uterus and fallopian tubes were conserved. Uterine repair and bilateral tubal ligation or abdominal hysterectomy are other surgical options for women who have completed their reproductive functions. 6 She was counselled on elective caesarean delivery for subsequent pregnancies so that she might avoid labour and its obvious consequences. It is believed that elective caesarean delivery at 36 weeks' gestation would make the possibility of spontaneous labour very remote while ensuring fetal maturation.
Because of the risk of uterine rupture during labour, women with prior adenomyomectomy should be offered elective caesarean delivery at term.