
Abstract
The epidemiology of Burkitt lymphoma (BL) has never been documented in Cameroon. Data were collected from 16 hospitals, the Delegation of Public Health and the regional pathologist in the Northwest province of Cameroon on all BL cases. The incidence of BL in this region is 5.9/100,000 children aged <15 years/year – the second highest incidence documented to date. Significant clustering was also identified in Ndop, a low-lying region with a high malaria endemicity, at 21.5 cases/100,000 children aged <15 year/year (P < 0.001).
Introduction
Burkitt lymphoma (BL) is endemic in sub-Saharan Africa. It is characterized by rapidly growing neoplasms, mainly of the jaw and abdomen, that are fatal within months without treatment. It typically occurs in children aged <15 years, in areas within 15º of the equator; at >15.6ºC, where there is >50 cm of annual rainfall and low-altitude. 1 The aetiology is thought to involve a genetic predisposition, malaria parasitaemia, Epstein-Barr virus (EBV), other arboviruses and Euphorbia tirucalli plants. 2
The Northwest province of Cameroon is 5–7º north of the equator, has a temperature of 18º–29ºC, an annual rainfall of 101.6 cm and an altitude ranging from 2500–3000 m in the mountains to 1100–1300 m in Ndop. 3 Malaria and EBV are endemic and euphorbia widely grown. 4 The province accommodated 745,009 children aged <15 years in 2005, who were cared for by 16 hospitals, 140 health centres and five private clinics. It is divided into 13 subdivisions (Figure 1). The successful treatment of BL at the Banso Baptist Hospital, Mbingo Baptist Hospital and Bamenda Provincial Hospital attract the vast majority of BL cases. It is through their high quality record keeping that suspicions arose of clustering in Ndop. 4 The present study was undertaken in order to determine the incidence and characteristics of BL in the Northwest province and whether any significant clustering existed.
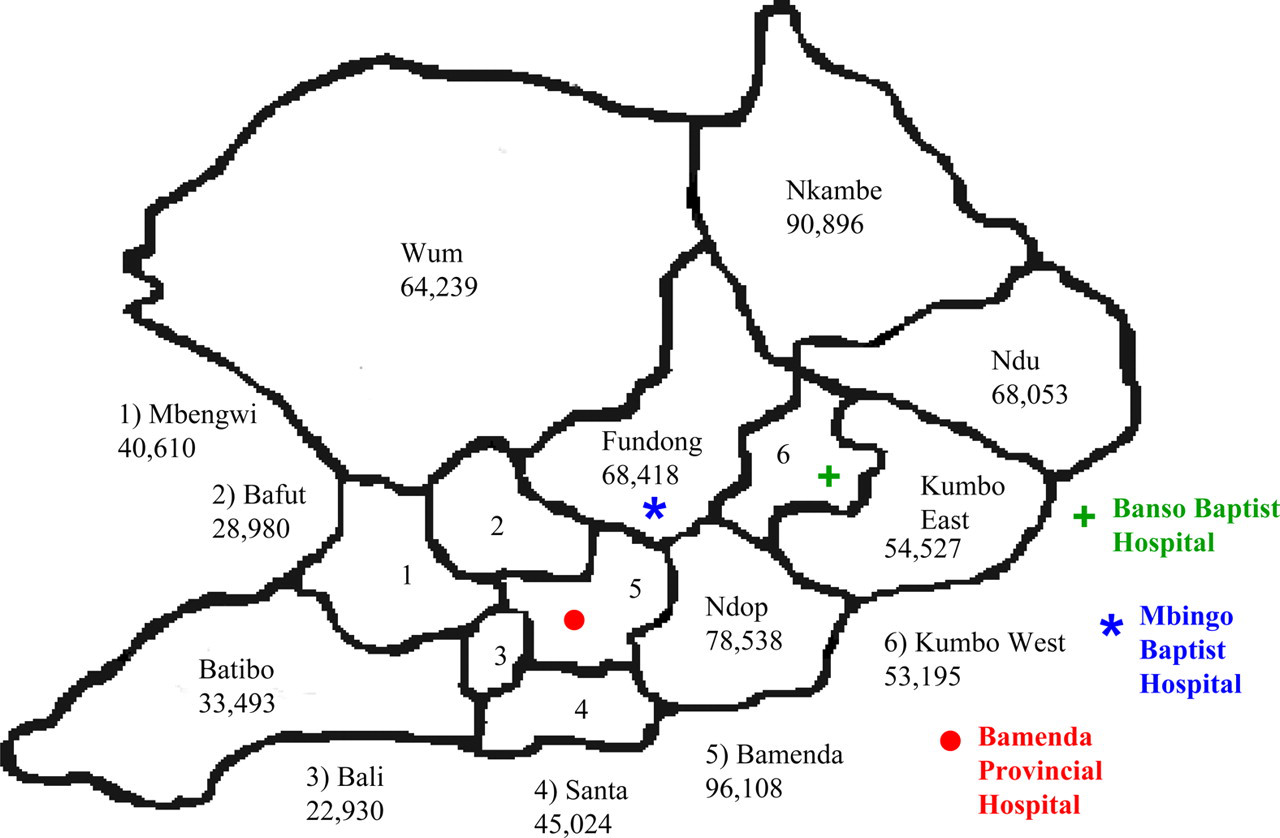
An outline map of the Northwest province of Cameroon indicating the provincial subdivisions, the three Burkitt lymphoma treatment hospitals and the estimated population of children under 15 years old in each subdivision
Methods
Data were collected from all 16 hospitals, the regional pathologist, private clinics and the Delegation of Public Health in the Northwest province on all BL cases. Health centres referred all cancer patients for hospital treatment. The aggressive nature of the cancer drives most cases to a health facility. Cases included had either a histological diagnosis or a clinical diagnosis of a fast-growing tumour, that responded to the Malawi 2002 protocol with complete regression within six chemotherapy doses, or, if they died before, an initial response of >50% reduction within three doses. 1,2 Patients who did not fulfill these criteria, but potentially may have had BL, were documented to allow for separate confirmed and potential incidences to be calculated.
Data were collected on the patientś home address, age, sex, tumour site and BL stage. 2005 was the only year when all hospitals had BL data available in order for us to document the incidence. However, data prior to and following 2005 were collected in order to create a larger sample size to enable us to analyse the characteristics of BL. Population and malaria data were provided by the Delegation of Public Health. Significant clustering was determined using a chi-squared test.
Results
In total, 211 cases of BL were identified from 8 February 2003 – 7 September 2006; 70% were confirmed histologically and 30% clinically. A further 24 potential cases were identified. Forty-four confirmed cases and 10 potential cases presented during 2005 and lived within the Northwest province. The confirmed incidence of BL in the Northwest province of the Cameroon is 5.9/100,000 children aged <15 years/year and a potential incidence 7.5/100,000 children aged <15 years/year. Ndop had 17 confirmed cases in 2005 and significant clustering at 21.5 cases/100,000 children <15 years/year (P < 0.001).
There were 57% males (120) and 42% females (89) (two unknown). The mean age was 7.9 years. Seventy-eight per cent (164) had abdominal involvement, 62% (131) head/neck involvement and 42% (88) both abdominal and head/neck involvement. There were 7% (15) St Jude stage I, 12% (25) stage II, 56% (119) stage III and 11% (24) stage IV (13% unknown).
Discussion
The incidence of BL in the Northwest province of Cameroon of 5.9/100,000 children aged <15 years/year exceeds all previously documented incidences, excluding one from Nigeria in 1960-1966 of 8.36/100,000 children aged <15 years/year (Table 1). 5 It is unlikely that our results represent an overestimation of the incidence as 70% of the cases were confirmed histologically and 30% clinically under a strict criteria. An underestimation is more likely as it is almost impossible to identify 100% cases in such an underdeveloped country.
The incidence of Burkitt lymphoma in sub-Saharan Africa 1
Significant clustering was apparent in Ndop with an incidence of 21.5/100,000 children aged <15 years/year (P < 0.001). A higher standard of record-keeping at Ndop Hospital cannot account for this, as all BL cases were identified at the three BL treatment hospitals and traced back to Ndop. However, the results are reliant on (1) the accuracy of the underlying child population data and (2) each subdivision having the same age distribution, as the chi-squared test assumes children in each subdivision have the same probability of getting BL, which varies with age.
Ndop is <1300 m, contains marshland, the Noun River and the Bamendjing Reservoir. Burkitt and Wright, Dalldorf et al. and Kitinya and Lauren, have shown a higher BL incidence in low-lying waterside regions within Uganda, Kenya and Tanzania, respectively. 6–8 Ndop had the highest percentage of paediatric cases under five years old diagnosed as malaria, and the second highest number of malaria cases under five years/1000 population; this coincides with studies by Burkitt et al. and Kafuko and Burkitt, who reported a relationship between malaria and BL. 9–11 However, Batibo subdivision also had high malaria indices, but there was no significant clustering. This could be explained by unknown environmental or genetic stimuli in Ndop predisposing to BL or inaccurate malaria data.
The characteristics of BL in the Northwest province of Cameroon are consistent with previous studies, except for the tumour site. All previous studies state the jaw as being most frequently involved; however in this study, 78% patients had abdominal involvement compared to 62% with head/neck involvement. 1 This is likely to be due to improved diagnoses through routine abdominal ultrasonography at the BL treatment hospitals.
Clinical studies are underway in the Northwest province of Cameroon in order to improve the management of BL; public health campaigns to promote earlier presentation of cases could improve survival rates still further. 4 An online cancer registry, POND4Kids, has been implemented to ensure ongoing monitoring of the problem. Ndop provides the ideal environment for further research into the aetiology of BL.