
Abstract
We present a case of disseminated histoplasmosis with acquired immunodeficiency syndrome (AIDS). A 38-year-old woman presented with fever, cough, dysphagia, significant weight loss and a loss of appetite. She also suffered from anaemia and cervical lymphadenopathy. A lymph node biopsy and a bone marrow aspirate showed intracellular yeast forms of Histoplasma capsulatum. She improved with parenteral amphotericin B and oral itraconazole. Even though histoplasmosis is not endemic in South East Asia and India, it should be kept in mind when evaluating AIDS patients in view of the current scenario of the pandemic.
Introduction
The aetiological agent of the fungal infection, histoplasmosis is a dimorphic fungus, Histoplasma capsulatum. It is mainly found in the soil in certain areas of the USA (i.e. the Mississippi and Ohio River valleys), sub-Saharan Africa, and Central and South America. 1–5 There have been frequent reports among AIDS patients but it has rarely been reported in India. This is the first case of disseminated histoplasmosis with AIDS reported from southern India.
Case history
A 38-year-old woman presented with fever and cough of eight days' duration, along with dysphagia of one week's duration, a significant weight loss and a loss of appetite. On examination she was pale. There was a 4×5 cm lymph node in the right posterior aspect of the neck which was firm and non-tender. Oral candidiasis was evident. Investigations revealed anaemia, thrombocytopenia and a normal total leukocyte count. Transaminases and alkaline phosphatase were moderately elevated. Malaria, dengue, leptospirosis and enteric fever were ruled out. The chest roentograph was normal. The possibility of tuberculous lymphadenitis/immunocompromised state was considered. The mantoux was negative. An HIV rapid assay was positive; this was confirmed by both an enzyme-linked immunoadsorbent assay and a Western blot test. Her immunoglobulin was negative for toxoplasmosis. A cervical node biopsy and a bone marrow test were done. The CD4 count was 21 cells/μL. The patient was started on cotrimoxazole as a prophylaxis against a possible pneumocystis jeroveci infection. The bone marrow (Figure 1) contained macrophages and a lymph node biopsy showed histiocytes packed with small oval yeasts surrounded by a clear halo. Yeast forms were para-aminosalicylic acid positive. Repeated blood and bone marrow cultures were sterile. Having confirmed the diagnosis of disseminated histoplasmosis, we started her on parenteral amphotericin B which was continued for a period of three weeks with a total cumulative dose of 515 mg. She responded quickly and became afebrile. She was later switched to oral itraconazole 200 mg twice daily. She was discharged on itraconazole. She was subsequently started on highly active antiretroviral therapy. On her first follow-up after one month she was asymptomatic.
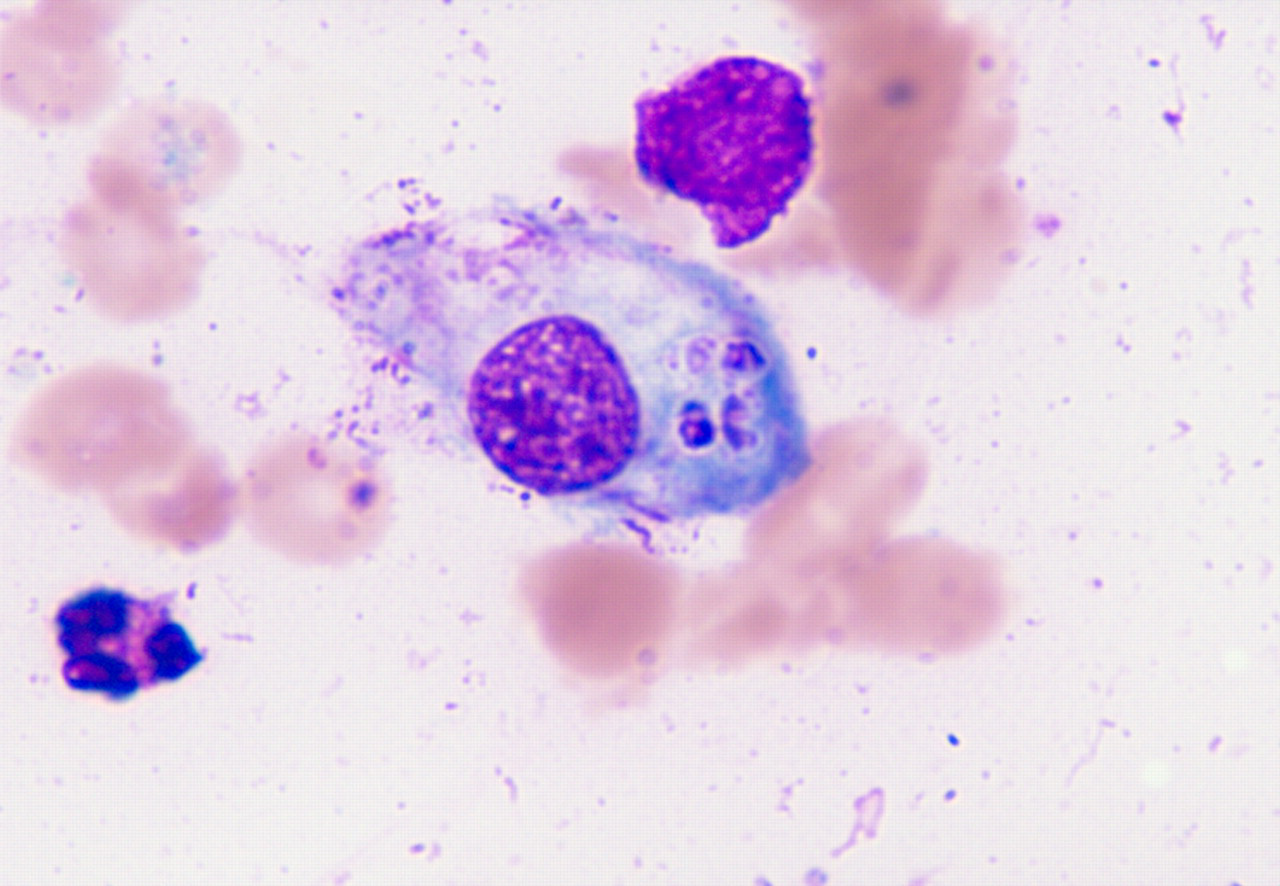
A Leishman stain showing intracellular yeast forms of Histoplasma capsulatum in a macrophage of a bone marrow smear (× 1000)
Discussion
Even with the emergence of HIV-AIDS and the associated spectrum of opportunistic infection, the detection of histoplasmosis among AIDS patients has not significantly increased. 5 In Africa, despite the current HIV pandemic, the detection of histoplasmosis remains rare and only 17 cases have been reported. 5
Disseminated histoplasmosis can involve the reticulo endothelial system, intestine, skin and liver, and may present with leucopenia and anaemia. 2 It is usually a late manifestation when associated with HIV infection and has an almost 20% mortality rate. 3, 5
There have been a total of four cases of disseminated histoplasmosis reported from India and ours is the first report of a case from the southern part of the country. The first case was a truck driver from West Bengal and the diagnosis was made from bone marrow aspiration and culture. 4 The next case was from Manipur and the diagnosis was made from both lymph node and bone marrow smears. 2 The third was from Assam and the diagnosis had been confirmed by fine needle aspiration cytology of the lymph node. 3 The most recent report was from Pune where the diagnosis was made by both bone marrow aspiration and a blood culture. 1
Considering the widespread occurrence of HIV-AIDS in the Indian subcontinent it is important to keep in mind the possibility of histoplasmosis among AIDS patients with fever and reticulo endothelial system involvement. It is suggested that bone marrow and lymph node evaluation be done with a high index of suspicion. 1 As it is extremely common in India, there is a significant bias towards making a diagnosis of TB. However, since histoplasmosis can masquerade TB, it is imperative to look very carefully for the organism in bone marrow and lymph node specimens.