
Abstract
Severe meconium aspiration syndrome is difficult to manage and has a high mortality in developing countries. Guidelines are available for the initial management. If the infant has been born through particulate meconium and is not vigorous, an inspection of the vocal cords by laryngoscopy is recommended. If meconium is seen at the cords it should, ideally, be sucked out of the trachea using an endotracheal tube as a suction device. However, as this needs a way of applying suction directly to the endotracheal tube it can be problematic. Commercially available equipment does exist, but in a resource-scarce setting, its cost could be prohibitive. We have adapted cheap suction connectors which can be adapted for this purpose.
Meconium aspiration syndrome (MAS) is caused by the inhalation of meconium into the amniotic fluid before, during or immediately after delivery. Most severe cases are due to problems in utero such as chronic asphyxia and infection. 1 It is not an uncommon problem, occurring in 11% (range 2 to 36%) of newborns delivered through meconium-stained amniotic fluid, which is seen in 14% (range 6 to 25%) of deliveries. 1–3
The immediate management of an infant who is not vigorous born through particulate meconium is to inspect the vocal cords using a laryngoscope and, if meconium is present, to aspirate it from the trachea using an endotracheal tube (ETT) as a suction catheter. 4 Ideally, the infant should be intubated with as large an ETT as possible and the suction should be applied directly while withdrawing and removing it. To do this it is, of course, necessary to connect the suction tubing to the ETT. Cole type shouldered ETTs have a side port to allow this but a disadvantage is that the shoulder only allows passage to just beyond the cords. Suction through a catheter passed down a large ETT is not ideal because material thick enough to cause airway obstruction is unlikely to be sucked up by a catheter small enough to pass down the tube. Intubating directly with a wide bore suction catheter is technically difficult because it is less rigid than an endotracheal tube and this cannot be overcome with an introducer.
The ends of ETTs are a standard size regardless of the ETT diameter. Commercially available (patented) equipment exists to connect them to suction tubing. However, Lautoka Hospital, Fiji, is a resource-scarce environment. We, therefore, prefer to make our own connectors. To do this we adapted standard suction connectors (Fiji Pharmac Connector/Polythene/Straight/00702/ID 6.0 mm/OD 8.0 mm/price 0.82 Fiji dollars [US$ 0.30]). Figure 1 shows the connector which has corrugated tapered wide and narrow ends (upper image). The wider end is cut at the fourth corrugation, effectively cutting it in half (middle image). The cut wider end now connects into the end of an ETT and the uncut narrow end connects into the suction tubing (lower image).
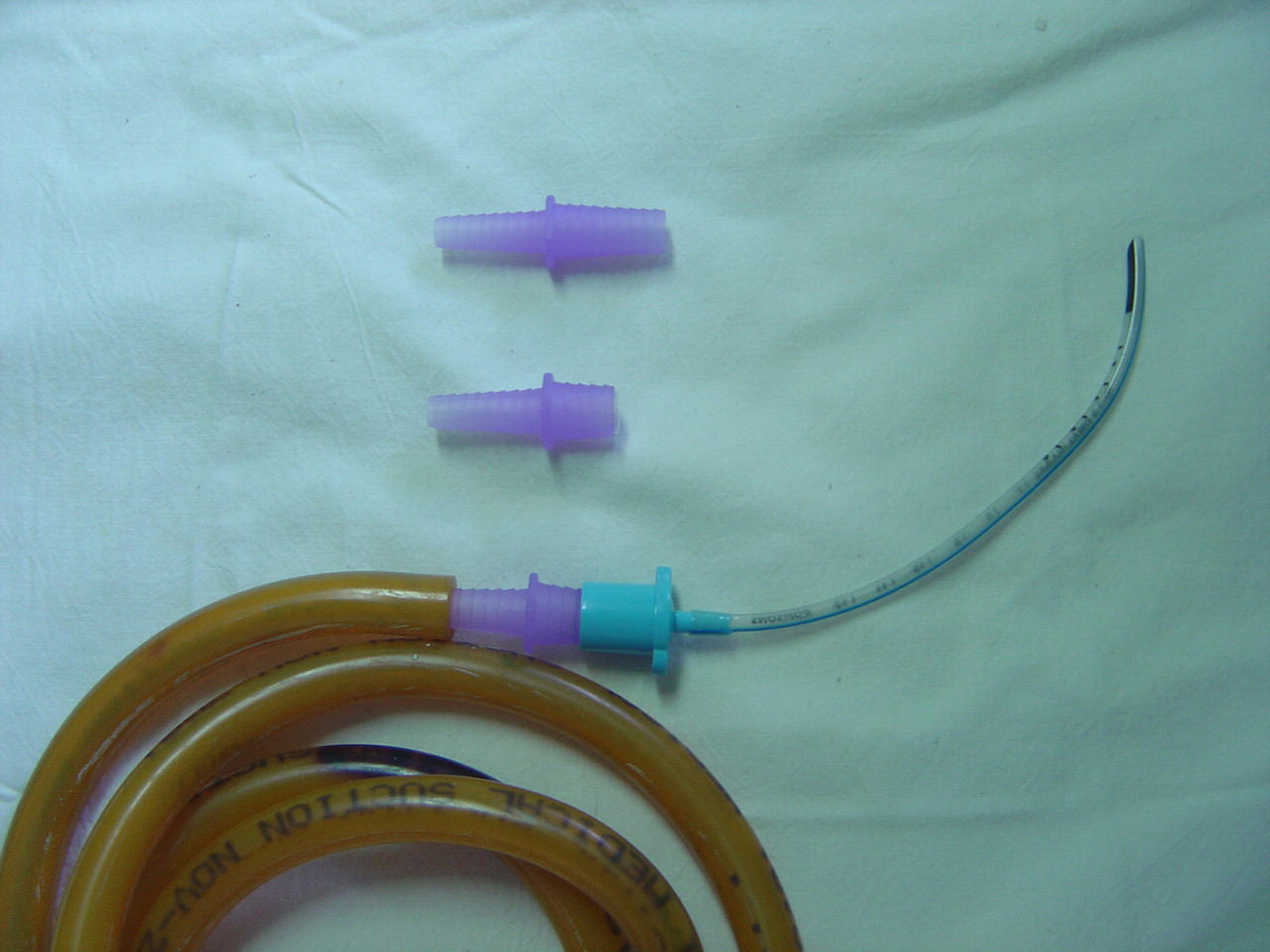
Adaption of a suction connector which can be attached to an endotracheal tube
The plastic of the connector is too thick to easily pierce to make a hole and therefore has no side (or thumb) port to allow for intermittent suctioning. We apply suction as we withdraw and remove the ETT in a smooth action lasting no longer than 2 seconds. We recommend a suction pressure of 80 mmHg or less. The connector can be autoclaved after use.