
Abstract
Chromoblastomycosis is a subcutaneous fungal infection caused by the traumatic inoculation of the skin with pigmented saprophytic moulds. Although infection is rarely fatal, it is characteristically chronic and can be complicated by lymphatic damage and malignant transformation. Despite a variety of treatment modalities, which are often combined and include long courses of antifungals, surgical excision and destructive physical therapies, it remains one of the most difficult deep mycotic infections to eradicate.
Epidemiology and aetiology
The pigmented (dematiaceous) fungi responsible for chromoblastomycosis are prevalent worldwide but infection is more common in the Tropics, with particular foci in India, Madagascar, Brazil, Venezuela, Mexico and the Dominican Republic. The most common aetiological agents are of the genera Fonsecaea, Phialophora and Cladophialophora, which are found as saprophytes in soil and plants. Fonsecaea pedrosoi is the most common agent found in tropical forests, such as the Amazon, as well as temperate regions of Latin America. Cladophialophora carrionii is the most important agent in dry countries and desert regions such as Australia, South Africa and Cuba (Table 1). 1,2
Principal causative agents of chromoblastomycosis 1
Investigations for chromoblastomycosis
Treatments for chromoblastomycosis
Clinical presentation
Chromoblastomycosis has a propensity to affect those who are barefoot, particularly agriculturists and labourers, and has a male and lower socioeconomic class predominance. The distal limbs are most commonly affected, although unusual body sites such as the genitalia and nose have also been described. 3 Disease progression is extremely slow and usually asymptomatic. Therefore, patients often seek medical treatment many years, or even decades, after acquiring the infection and developing skin lesions. Early lesions consist of only a single papule or nodule. Over years they enlarge, forming plaques with a characteristic verrucous appearance (Figure 1). Disease is usually localized but satellite lesions can develop as a result of autoinoculation from scratching or from lymphatic dissemination. As lesions extend they leave areas of sclerotic or keloidal scarring. Complications include secondary bacterial infection, ulceration, secondary lymphoedema, and, rarely, the development of squamous cell carcinoma. Lymphoedema itself can predispose to attacks of cellulitis. Extension of infection to underlying muscle and bone is rare and usually only occurs in association with immunosuppression. 2,4 The principal differential diagnosis of chromoblastomycosis in the Tropics is verrucous variants of tuberculosis, sporotrichosis and leishmaniasis.

Verrucous plaque over elbow with characteristic ‘black dots’
Diagnosis
The clinician can confirm the diagnosis easily by direct microscopy of a scraping taken from the characteristic black dots visible on the surface of skin lesions (Figure 1). These black dots represent transepidermal elimination of fungae. A positive direct examination of scrapings in 10% potassium hydroxide will demonstrate thick-walled, multi-septate, brown sclerotic cells that are pathognomonic of chromoblastomycosis, irrespective of the causative species (Figure 2). These are known alternatively as ‘copper pennies’, ‘Medlar bodies’ or ‘muriform cells’. The fungal agents are typically slow-growing and culture may be inconclusive due to poor morphological differentiation. Polymerase chain reaction (PCR) has been developed for the identification of Fonsecaea and Cladophialophora carrionii. 5,6 Serological tests such as ELISA can be useful in evaluating therapy response, but like PCR it is not widely available in most endemic settings. 7 A biopsy demonstrates the typical sclerotic bodies within a granulomatous infiltrate (Table 2).
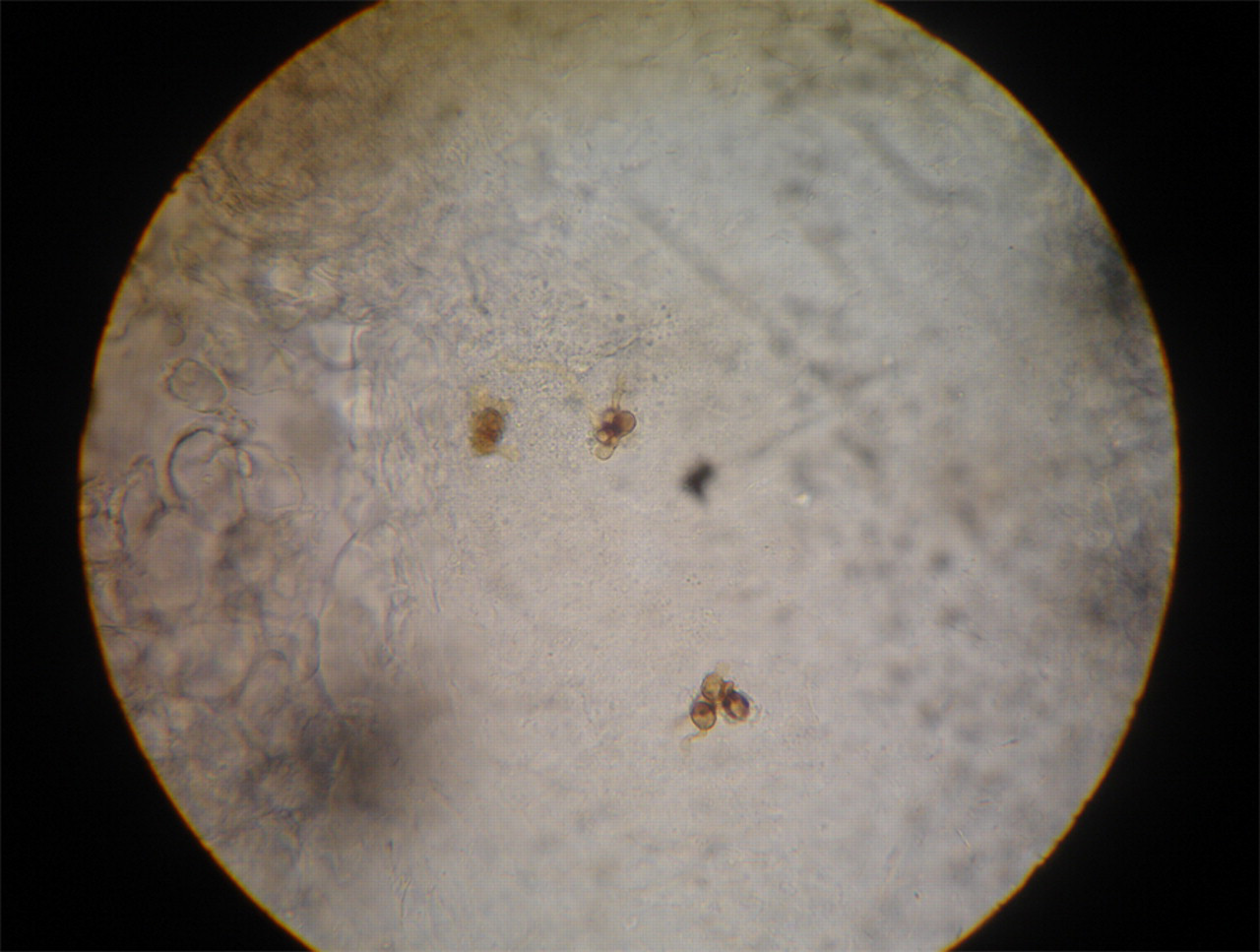
Direct examination in a potassium hydroxide mount of skin scrapings demonstrate characteristic ‘copper pennies’ (×400 magnification)
Treatment
Cure rates for chromoblastomycosis are low and range from 15% to 80%. Chronic and extensive disease is particularly resistant to treatment. In addition, F. pedrosoi, the most common aetiological agent of chromoblastomycosis, is less sensitive to antifungal chemotherapy than C. carrionii or P. verrucosa. 8 The goal of treating small and early lesions should be cure. However, in the case of extensive infection a more realistic goal might be to reduce disease, control spread and prevent complications. Clinical cure is defined as complete resolution of lesions with scarring, and mycological cure is defined as negative microscopy and culture.
Drug therapy consists of long courses of high dose antifungals. Unfortunately, there are no comparative trials of their use in chromoblastomycosis. First-line agents are itraconazole (200–400 mg daily) and terbinafine (500–1000 mg daily), which have both demonstrated good in vitro activity against causative species of chromoblastomycosis. 9,10 They are given for a minimum of 6–12 months, preferably at the higher dose if tolerated. 11–13 Pulse itraconazole (200 mg twice daily for one week every month) has demonstrated comparable efficacy to daily itraconazole, and the consequent reduction in its cumulative dose has the dual advantage of reducing risks of long-term drug therapy and bringing down its cost. 14 Combination therapy with itraconazole and terbinafine is recommended if it is affordable. 15 It is well-tolerated and its enhanced efficacy may be accounted for by its synergistic effects, which have been demonstrated in recent in vitro studies. 16,17 Ketoconazole has low efficacy against chromoblastomycosis and cannot be given at high doses for long periods of time because of its hepatotoxic potential. 8 Fluconazole and amphotericin B are also not recommended as in vitro studies have shown that it has poor activity against dematiaceous fungi. 9 Flucytosine was an early treatment for chromoblastomycosis. 18 However, it is highly toxic and is associated with high levels of resistance. It is rarely used now except for the treatment of cases resistant to first-line agents. The new second generation broad-spectrum triazoles such as posaconazole and voriconazole are promising drugs for treating deep cutaneous mycoses, but experience to date is limited because of their prohibitive costs. A single study demonstrated cure with long-term posaconazole in five out of six patients with chromoblastomycosis refractory to standard antifungal therapies, and long-term therapy (up to 34 months) was well tolerated. 19 Drug therapy should be continued for several months after cure in order to prevent relapse, which is more common for extensive disease.
Drug therapy can be combined with surgery or physical destructive treatments such as cryotherapy or thermotherapy. Excision of small, localized lesions with wide surgical margins can be very successful. 8 Ideally, antifungal chemotherapy should be given before surgery in order to reduce the size of the lesion, and should be continued afterward to reduce any risk of recurrence. Physical treatment modalities have the advantage that they are inexpensive and easy to administer. They are also a useful option for patients unable to take systemic medication. Cryotherapy, involving the application of liquid nitrogen to lesions, produces low temperatures, which freezes and destroys diseased tissue. Multiple lesions may be treated as tolerated and treatment can be combined with antifungal chemotherapy. Cryotherapy of large lesions is usually done in stages. However, treatment of smaller lesions is usually more successful and sometimes requires only a single application. 4,20,21 Thermotherapy involves the application of local heat to produce controlled temperatures ranging from 42°C to 45°C. Various devices, such as benzene pocket warmers and pocket handkerchief-type warmers, have been used. The few reports of its use originate from Japan and demonstrate high efficacy as monotherapy. 22,23 Thermotherapy in combination with antifungals may reduce treatment duration and improve efficacy (Table 3).
Conclusion
The diagnosis of chromoblastomycosis may be confirmed easily at the first clinical visit by the direct microscopic examination of scrapings of a suitable skin lesion. Treatment choice must be tailored according to the aetiological agent, extent of disease and its location, and any co-morbidities which preclude long-term antifungal chemotherapy. Combination high-dose intraconazole and terbinafine therapy is recommended in conjunction with surgery and cryotherapy of small lesions.