
Abstract
The objective of this study was to compare complications and effectiveness of induction after vaginal and sublingual administration of misoprostol for labor induction in women with intra-uterine fetal death (IUFD). In a district hospital in Ghana, 23 women with IUFD who underwent labor induction with sublingual misoprostol were compared with a control group of 21 women who received vaginal misoprostol. In the vaginal group 28.6% had one or more complications compared to 21.7% in the sublingual group. In the sublingual group three inductions did not lead to delivery within 48 hours (13%), compared to four in the other group (19%). The mean induction-to-delivery time in the sublingual group was 13 hours and 17 hours in the vaginal group. In this study, both sublingual and vaginal misoprostol were safe and efficient for labor induction in women with IUFD. However, more research on larger numbers of patients is needed, in order to compare complications.
Introduction
Intra-uterine fetal death (IUFD) is an obstetric situation which often requires the induction of labour. The definition of IUFD is the death of the fetus in utero occurring after 20 weeks of gestation. It occurs in 1% of all pregnancies. 1 Safe delivery for women is a major challenge, particularly in developing countries such as Ghana. The vast majority (90%) of women with IUFD deliver spontaneously within three weeks after fetal death, indicating that expectant management might be a good option. However, induction of labour is indicated for the prevention of complications such as diffuse intravascular coagulation (DIC), with its inherent risk of haemorrhage, need for blood product transfusion and maternal death. The risk of clotting defects due to DIC is 10% if the patient remains undelivered after four weeks. 2 The psychological aspects of carrying a macerating fetus can also be a reason for the induction of labour.
Current methods of labour induction include the use of misoprostol, a synthetic analogue of prostaglandin E1. Misoprostol is effective in the induction of labour but further research is required in order to assess the complications and side effects. 3–6 Complications described in previous studies are: the need for caesarean section; retained placenta; oxytocin augmentation; postpartum haemorrhage; fever; and uterus rupture. 1,7–9 Side effects, such as nausea, vomiting and fever, have also been described. 10
The most favourable method for the administration and the optimal dose of misoprostol has not yet been established. Several studies indicate that oral misoprostol is less effective and results in more side effects than intravaginal doses. 7–9 Sublingual misoprostol is another route of administration. Since the pharmacokinetics are different for sublingual and vaginal misoprostol, differences in efficacy and side effects need to be compared. So far, the sublingual administration of misoprostol has only been evaluated in a few trials. The pharmacokinetic advantages are described as rapid onset of action, prolonged activity, greater bioavailability and that it is a less invasive route than vaginal administration. 9 It is suggested that sublingual administration of misoprostol is more effective as it gives shorter induction-to-delivery intervals, greater success rates of delivery within 48 h and better cervical dilatation than vaginal misoprostol. 3,5,11 Patient acceptability is also higher in women induced with misoprostol given sublingually compared to vaginal administration. 3,5,12 However, one study reported that vaginal administration in a second trimester termination of pregnancy has a significantly higher success rate for delivery within 48 h. 13
The aim of this study was to compare complications and efficacy of sublingual and vaginal methods of the administration of misoprostol for labour induction in IUFD.
Methods
This study was performed at the Holy Family Hospital, Berekum, Ghana, a 164-bed district hospital which serves an estimated population of 110,000 people. The hospital receives referrals from five maternity homes in the district and from neighbouring districts. Around 1600 women per year deliver in the hospital with a still birth rate of 3%.
All the women who suffered a still birth during 2006 and 2007 were analysed and only those who delivered a still birth after being admitted for induction of labour for IUFD were included in this study. Women who underwent labour induction during the current regimen of sublingual misoprostol 200 mcg once in 24 h were considered as cases and were compared with women who received misoprostol according to the previous regimen of 200 mcg once in 24 h vaginally (controls). All women received 10 units of oxytocin intramuscular after delivery. The women in the vaginal group received oxytocin per infusion after delivery when needed. In the sublingual group all women received oxytocin per infusion after delivery. As such, all data for the vaginal group were collected retrospectively and half of the data from the sublingual group were collected prospectively. Both groups were assessed on the following outcome measures: complications (caesarean section, mechanical delivery, retained placenta, postpartum hemorrhage, postdelivery anaemia, septicaemia), side effects, induction-to-delivery time and delivery within 48 h. Postpartum haemorrhage was defined as blood loss of more than 500 mL after delivery.
An Hb of lower than 11.0 g/dL was considered as anaemia. Statistical analysis of the data was performed in Statistical Package for Social Sciences (Version 14.0 SPSS). Means were compared using the unpaired t-test, and percentages were compared using chi-square tests, or Fisher's exact tests, and odds ratios (OR) and confidence intervals (CI). A P value <0.05 was considered as significant.
Results
We included 44 women with IUFD who had received misoprostol for induction of labour in 2006 or 2007. Twenty-one of these cases received 200 mcg misoprostol for labour induction vaginally and 23 women received 200 mcg sublingually. No differences were observed between the two groups concerning age, obstetric history, the duration of gestation and presenting part of the fetus at the time of the induction (Table 1).
Comparison of clinical data in the group of patients receiving vaginal misoprostol and the group receiving sublingual misoprostol
In the group of patients who received vaginal misoprostol 28.6% had one or more complication compared to 21.7% in the group who received sublingual misoprostol (OR = 1.44, 95% CI = 0.18–2.73) (Figure 1).
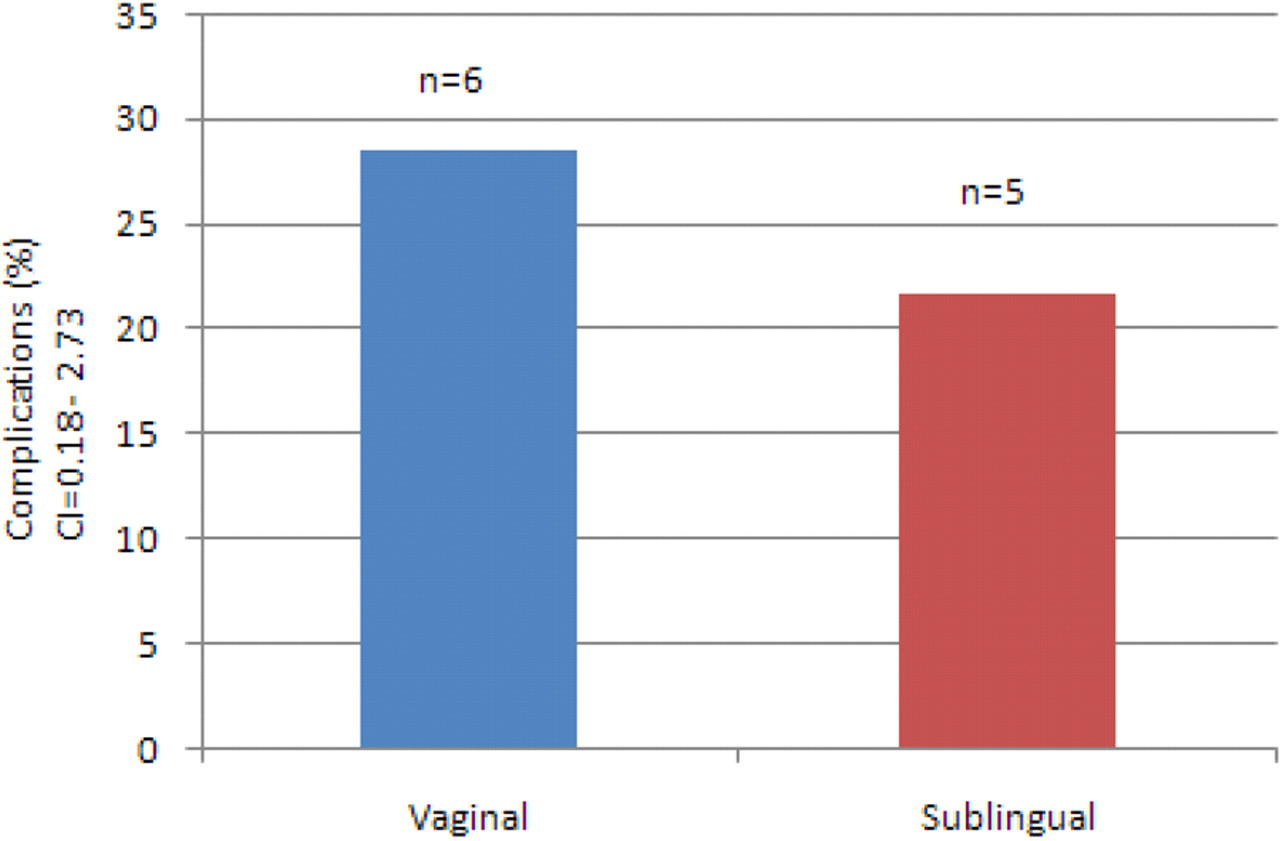
Number of patients having any complication in the group receiving vaginal misoprostol and the group receiving sublingual misoprostol
No differences between both groups were found for complications such as caesarean section, mechanical delivery, postpartum haemorrhage, postdelivery anemia and septicaemia. In the vaginal group retained placenta occurred more often (14%) than in the sublingual group (4%) (OR = 3.67, 95% CI = 0.26–2.85). In both groups none of the subjects required blood transfusion, there were no mortalities and no uterus ruptures reported (Table 2).
Comparison of complications in the group of patients receiving vaginal misoprostol and the group receiving sublingual misoprostol.
In Figure 2, failed inductions are depicted: in the sublingual group three inductions did not lead to delivery within 48 h (13%) compared to four in the other group (19%) (OR = 1.50, 95% CI = 0.12–3.25). The induction-to-delivery time ranged from 2 h and 15 min to 14 days in the vaginal group and from 10 min to 6.5 days in the sublingual group. When failed inductions (no delivery within 48 h) and caesarean sections are excluded, mean induction-to-delivery time in the vaginal group was 13 h compared to 17 h in the sublingual group (P = 0.39; Figure 3).
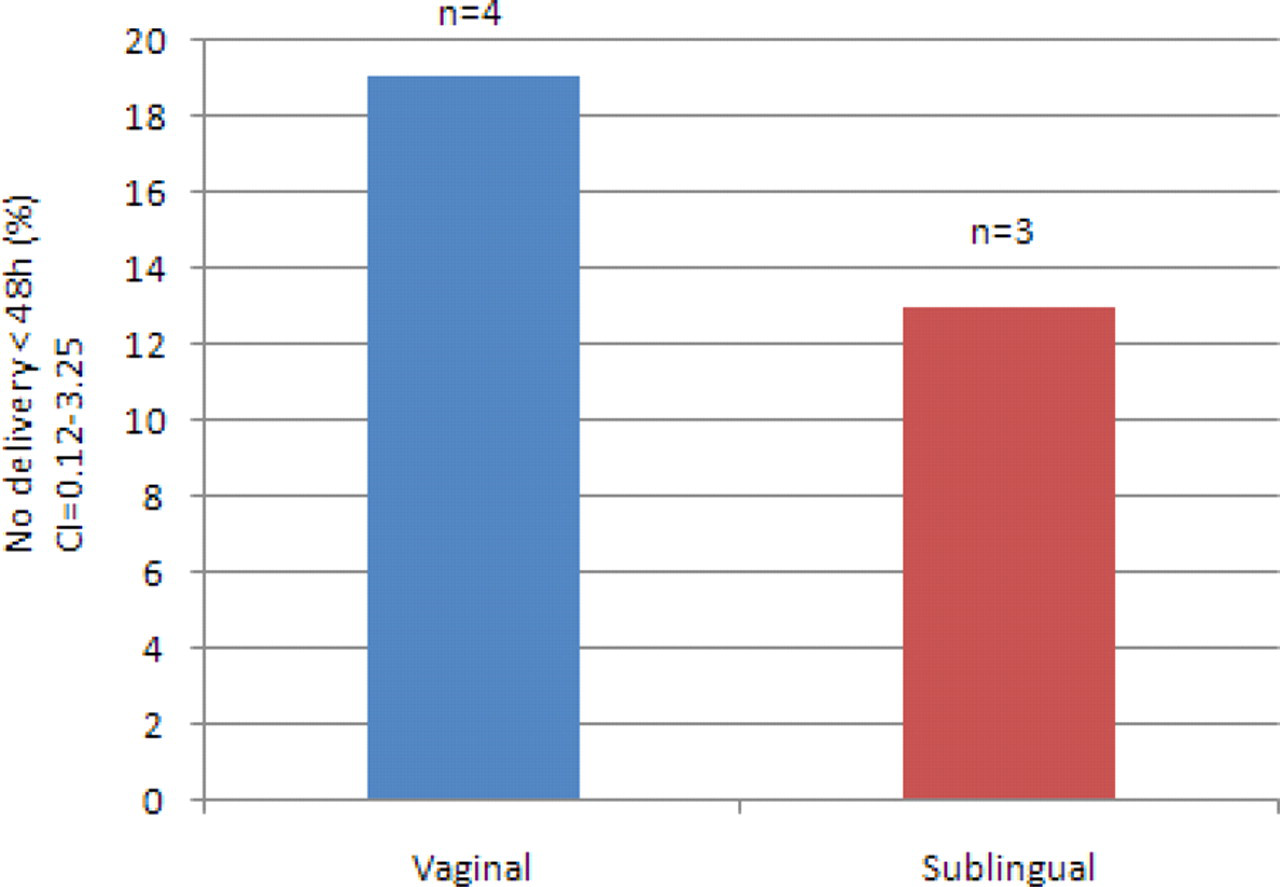
No delivery within 48 hours in the group of patients receiving vaginal misoprostol and the group receiving sublingual misoprostol
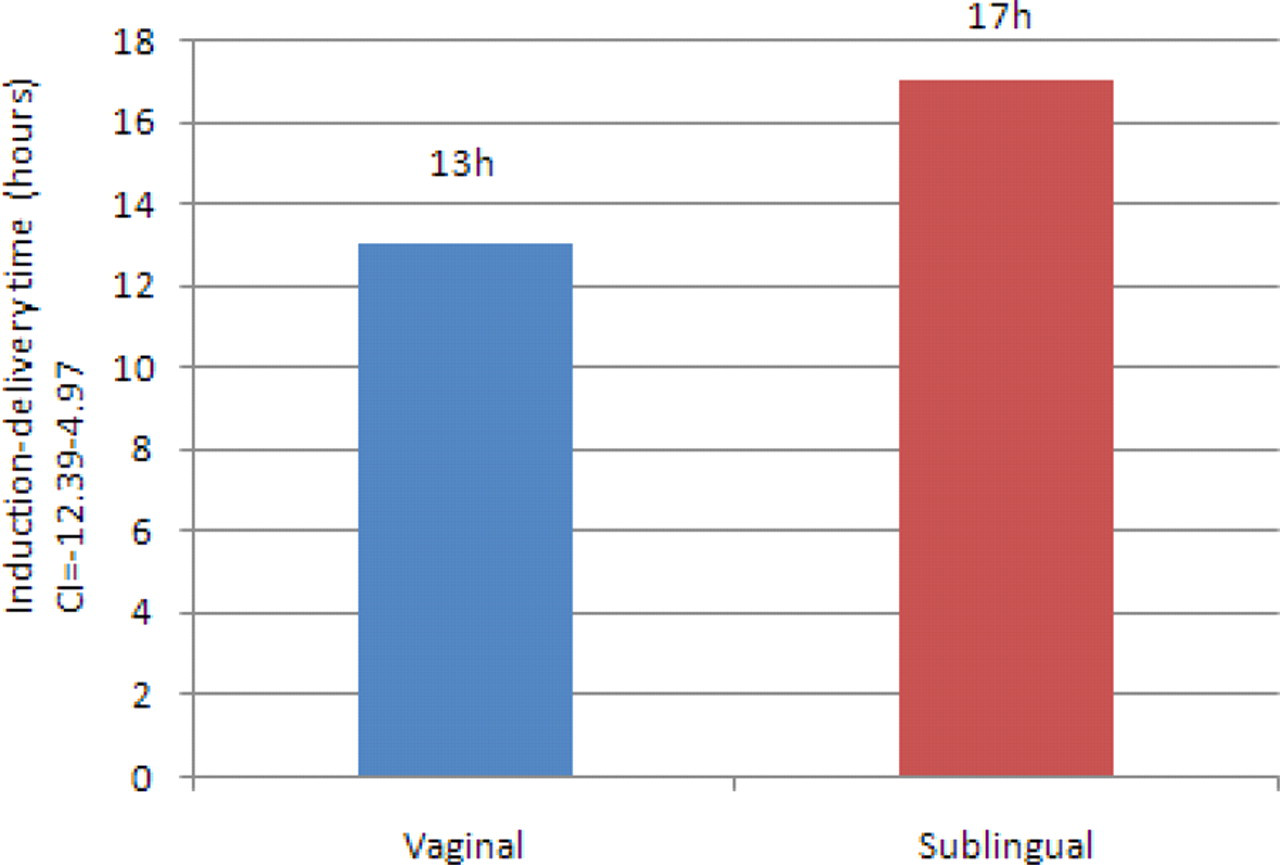
Induction-to-delivery time in the group of patients receiving vaginal misoprostol and the group receiving sublingual misoprostol
The amount of oxytocin ranged from 10–230 units in the vaginal group, of whom 52% received oxytocin (mean 24 units) and from 10–100 units in the sublingual group, of whom all received oxytocin (mean 36 units; P = 0.31).
Discussion
Sublingual misoprostol is a safe and effective way to induce labour in women with IUFD. There were no differences in complications or number of failed inductions between vaginal and sublingual administration of misoprostol. We did not find serious complications after induction of labour for IUFD with misoprostol. Complications that were found are comparable to complications described in other studies, 1,7–9 except for the number of patients with retained placenta after vaginal misoprostol, which is higher than in a previous study (14% versus 3.3%). 8
The success rate of delivery within 48 h was 87% in the sublingual group and 81% in the vaginal group. In the previous studies higher success rates of 93%–100% were described for delivery within 48 h after vaginal insertion of misoprostol. These studies used comparable total doses of misoprostol for the induction of labour. 8,14,15 One study reported a success rate within 48 h of 95% after vaginal insertion and 91% after sublingual administration. 13 However, the dose used in these series was up to ten times higher than the dose used in this study.
The mean induction-to-delivery time in the vaginal and sublingual group was 13 h and 17 h, respectively. This difference was not significant. In the group induced with vaginal misoprostol there were three breech presentations, compared to none in the sublingual group. This might have prolonged the mean induction-to-delivery time in the vaginal group. The results are comparable with outcomes described in other studies. Induction-to-delivery time for intravaginal insertion of misoprostol ranges from 12.0 h to 19.8 h; 8,11,13–17 for sublingual administration the range is from 10.5 h to 13.8 h. 11,13
The dose of 200 mcg in 24 h used in this hospital is relatively low. In previous studies, a large range of doses of intravaginal and sublingual misoprostol used for the induction of labour are described, ranging from 100 mcg (12-hourly) to 400 mcg (3-hourly). 8,11,13–17 Furthermore, different dosages can be used at different gestational ages. One study recommended the following dosages for the vaginal use of misoprostol in IUFD: 200 mcg (6-hourly) for a gestational age of 13–17 weeks; 100 mcg (6-hourly) for 18–26 weeks; and 25–50 mcg (4-hourly) for 27–43 weeks. 1
Side effects, such as nausea or vomiting, were not found in the patient records, which meant they were either not experienced or not recorded. In prospectively reviewed cases no side effects were reported by the patients. For this reason we consider that side effects were not a major problem for the women included in our study.
This study, performed in a rural hospital in Ghana, is partly a retrospective research, with the disadvantage that documentation was sometimes incomplete. We analysed all women with IUFD in the hospital in two years but the included groups were relatively small and not randomized. However, the two groups were comparable in age, gestational age and parity. The patients' preference for vaginal or sublingual route of administration was not investigated.
Furthermore, the additional use of oxytocin was not comparable for both groups. In this study, the policy regarding the use of oxytocin changed with time. All patients in the sublingual group received additional oxytocin after labour. In the group of patients who received vaginal misoprostol, oxytocin was only added when needed. Many different regimens for oxytocin are described. The additional use of oxytocin is described as a negative outcome measure in a previous study. 16 Other studies compared the use of oxytocin with the use of misoprostol 8,18 It is difficult to determine the influence of oxytocin on the results of the current study but it may have influenced the results of complications such as retained placenta and postpartum haemorrhage.
Not much literature on the use of sublingual misoprostol for induction of labour is available. Previous studies are based on different designs and, therefore, the misoprostol dosage, gestational age and reason for induction are not comparable. Furthermore, due to the small number of patients, results were not significant. More prospective research on the use of sublingual misoprostol is desirable in order to assess the safety, side effects, the optimal dose for different gestational ages and to confirm the findings of this study. In conclusion, sublingual and vaginal misoprostol are both safe and efficient for the induction of labour in IUFD. There were no differences in complications and induction-to-delivery times. The sublingual route might be preferable as it is easier.