
Abstract
Tuberculosis (TB) of the cervix is a rare disease. We describe two cases of tuberculous cervicitis with variable clinical presentation. In one case, a young woman presented with primary infertility and secondary amenorrhoea. The other is a perimenopausal woman with irregular vaginal bleeding and postcoital blood-stained discharge. The diagnosis was confirmed on histopathological examination of the endocervical curettings and a cervical biopsy. The patients were given six months of anti-tuberculous therapy and responded well.
Introduction
Genitourinary tuberculosis (TB) is more prevalent in developing countries. Fallopian tubes and ovaries are commonly involved. Rarely, other pelvic organs like the vagina, vulva, myometrium and cervix may be involved. Cervical TB accounts for 0.1–0.65% of all cases of TB and 5–24% of genital tract TB. 1 Cervical TB is usually not suspected clinically and, in a postmenopausal woman, it may simulate carcinoma. Here we present two cases of cervical TB with variable clinical presentation.
Case History
Case 1
A young 20-year-old woman with primary infertility presented with a complaint of secondary amenorrhea. There was no history of bleeding per vaginum, itching or any local lesion. There was no personal history of, or exposure to, TB. Gynaecological examination revealed an unhealthy looking cervix which was grossly erythematous, congested and bled on touch. There was white-coloured discharge which was foul-smelling. Hysterosalpingography revealed a normal uterus with no adhesions and bilateral patent fallopian tubes. Endocervical curettings were sent for histopathological examination. On microscopic examination the curettings comprised of mucus and endocervical tissue revealing features of tuberculous endocervicitis. There were foci of caseating and non-caseating granulomas along with Langhans' giant cells, although staining for acid-fast bacillus (AFB) was noncontributory. The patient responded to antitubercular treatment.
Case 2
A 50-year-old mutipara woman presented with irregular vaginal bleeding and postcoital blood-stained discharge for the previous eight months. There was no history of contact with TB. Gynecological examination revealed mixed discharge in the vagina. She had an unhealthy cervix with ulceration and bleeding. A cervical biopsy was taken. A histopathological examination revealed ulcerated fragments of cervix with severe chronic active inflammation, along with multiple epithelioid cell granulomas and Langhans' giant cells in the stroma (Figure 1). AFB were demonstrated with Ziehl-Neelson stain.
Cervical biopsy showing endocervical lining and caseating granulomas in the stroma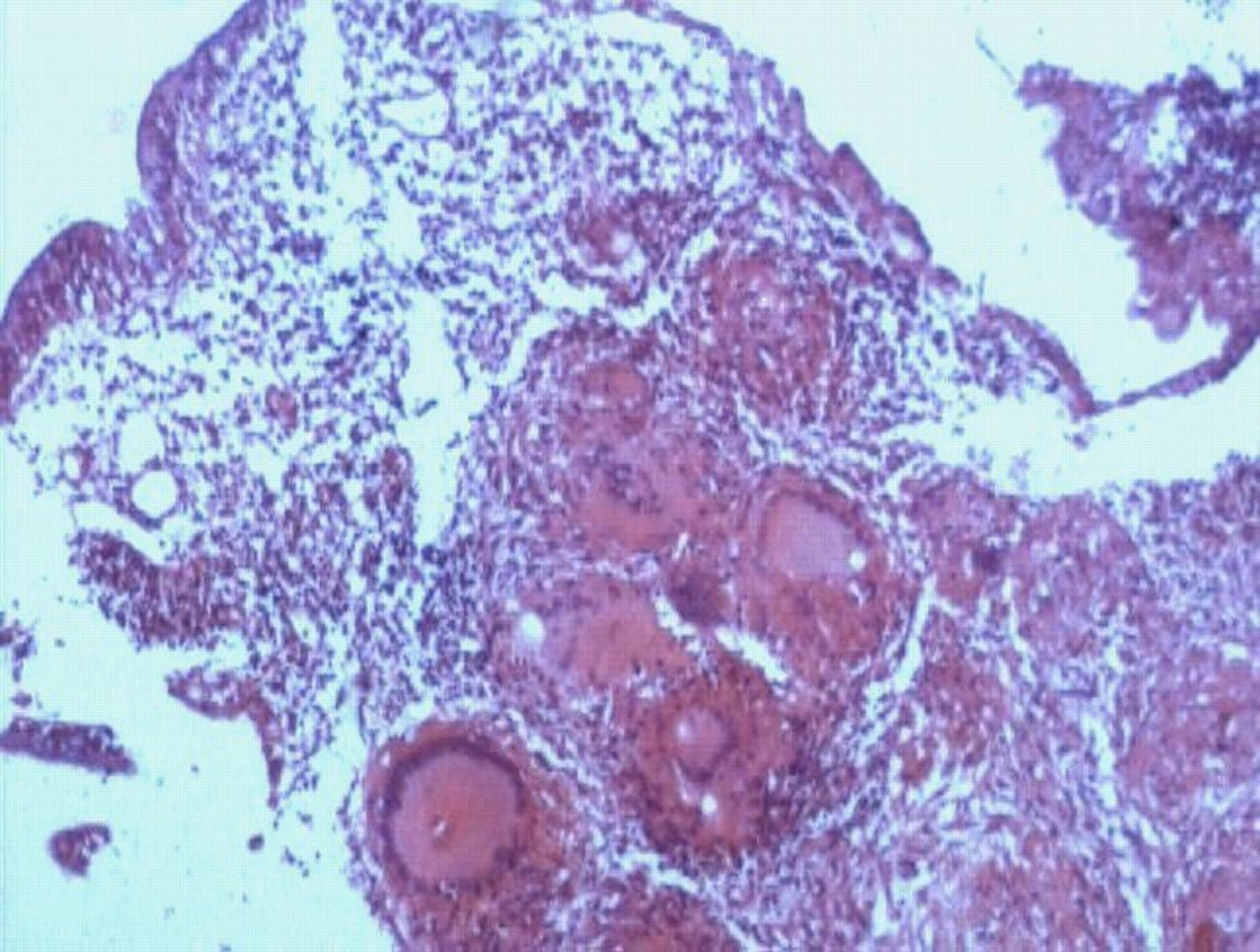
Discussion
TB of the cervix is a rare disease. Cervical TB is almost invariably secondary to tuberculous salpingitis and endometritis. In rare cases, cervical TB may be a primary infection introduced from a partner with tuberculous epididymitis or other genitourinary diseases. 2 Sputum used as a sexual lubricant may also be a route of transmission. 3
The common presentations in TB of the female genital tract are amenorrhoea, menstrual irregularities, infertility, vaginal discharge and postmenopausal bleeding. The gross appearance of the tuberculous cervix is highly variable. It may present as papillary, ulcerative, interstitial, miliary, endocervical or polypoid forms.
Histologically, tuberculous cervicitis is recognized by the presence of multiple caseating granulomas or tubercles. Heavy lympho-plasmacytic infiltrate is present at the rim of the tubercles. However, granulomatous lesions may also be encountered in lymphogranuloma venereum, sarcoidosis, schistosomiasis and foreign body giant cell granulomata to suture, crystal or cotton. 4
The diagnosis is usually made by a histological examination of a cervical biopsy specimen. Unequivocal diagnosis requires demonstration of AFB with Ziehl-Neelson staining. However, staining for AFB may not be positive in every case. The presence of granulomata on cervical cytological specimens has been documented. 5 Isolation of the mycobacterium is the gold standard for diagnosis. Approximately one third of cases are culture negative. Therefore, the presence of typical granulomata is sufficient for diagnosis if other causes of granulomatous cervicitis are excluded or a primary focus identified. 1
To summarize, the diagnosis of female genital TB presents a problem, as in many cases, the clinical symptoms and physical examination give no indication. The definitive diagnosis is based on a histological demonstration of the characteristic lesion or on positive bacterial evidence.