
Abstract
The increasing awareness of the worse than expected outcome after typhoid ileal perforation (TIP) prompted us to prospectively prognosticate patients with the help of the Jabalpur prognostic score (JPS), a simplified scoring system for peptic perforation peritonitis (PPP). Eighty-two consecutive patients with TIP were studied from May 2005 to August 2008 in the Department of Surgery, NSCB Government Medical College, Jabalpur (MP), India. Six parameters used in the JPS were recorded: age, heart rate, mean blood pressure, serum creatinine, any co-morbid illness and perforation-operation interval. JPS correlated with morbidity and mortality in TIP patients and, as the score increased, so did the morbidity and mortality. Survivors had a significantly lower mean score (3.86 ± 2.23) than non-survivors (7.94 ± 3.6; P < 0.001). Expectedly, TIP patients had worse outcome, stage by stage, than PPP patients. JPS can be easily modified for TIP (JPS-TIP) and can be easily used for its prognostication.
Introduction
Typhoid ileal perforation (TIP) is the second most common cause of generalized peritonitis in the developing countries after perforated peptic ulcer. Factors predicting the outcome in cases of perforation peritonitis are well documented and have been used in the construction of various scoring systems. 1,2 The Jabalpur scoring system (JPS), a simple, economical and user-friendly system, was developed for use in the developing countries and has been effectively used for cases of perforated peptic ulcers. 3 An increasing awareness of the worse than expected outcome after TIP prompted us to prospectively prognosticate these patients with the help of JPS.
Methods
The present prospective study was undertaken for 82 consecutive TIP patients in the Department of Surgery, NSCB Government Medical College, Jabalpur (MP), India, from May 2005 to August 2008. The diagnosis was made using a combination of history, clinical examination, radiological imaging and emergency exploratory laparotomy. Six parameters used in JPS were recorded: age, heart rate, mean blood pressure, serum creatinine, any co-morbid illness and perforation-operation interval (Table 1).
Jabalpur prognostic score
Co-morbid illness, if present, is given a score = 5
Total score = perforation-operation (P-O) interval score + age score + blood pressure (BP) score + heart rate score + creatinine score + co-morbidity score
Co-morbid illness was defined as per the APACHE-II scoring system, with emphasis on the respiratory system due to high incidence of pulmonary infection/tuberculosis in our patients. All patients underwent closure of the perforation (for single perforation)/resection of affected segment (for multiple perforations), proximal ileostomy, thorough peritoneal lavage and bilateral abdominal drainage.
The duration of the hospital stay, complications and/or death were recorded. Mortality was defined as death in hospital during the episode of perforation-peritonitis. Predicted mortality and morbidity by JPS (taking peptic perforation peritonitis [PPP] patients as controls) was compared with actual mortality and morbidity. The statistical analysis was done using SPSS 11.5 software. The appropriate univariate, bivariate, multivariate or logistic regression analysis was carried out using the Student's t-test for the continuous variables and two-tailed Fisher's exact test or chi-square test for categorical variables. The critical level of significance of the results was considered at 0.05 levels.
Results
The mean age of the TIP patients was 30.02 years (range 14–62). There were six times as many males as females (70:12). The mean duration of a hospital stay was 15.18 days (range 1–48). Seventeen (20.7%) patients died and 43 (52.4%) patients had complications, including mortality. Multiple organ dysfunction syndrome (n = 10) and severe respiratory infection (n = 11) were the most common causes of mortality. One patient had entero-cutaneous fistula proximal to ileostomy, which required revision. Superficial wound infection (n = 14) and wound dehiscence (n = 6) were the most common complications and were responsible for a longer hospital stay.
Of the six risk factors constituting JPS, age, serum creatinine, perforation-operation interval and co-morbid illness were significantly associated with mortality and morbidity (Table 2). In addition, severe respiratory infection was observed in 24 patients, 14 of whom died (P = 0.009). The mortality rate was 0% when the perforation-operation interval was <24 h, 11% (n = 4/36) when the interval was 25–72 h, 55.5% (n = 5/9) between 97–120 h and 100% (n = 4/4) when the interval was >120 h (Table 3). Overall, the JPS (range 3–16) correlated with morbidity and mortality in TIP patients, and as the score increased, so did the morbidity and mortality (Table 4).
Correlation of risk factors with mortality and morbidity
Morbidity and mortality in relation to Jabalpur prognostic score
Comparison of morbidity and mortality in peptic perforation peritonitis (PPP; n = 140) and typhoid ileal perforation (TIP; n = 82)
JPS, Jabalpur prognostic score
Survivors had a significantly lower mean score (3.86 ± 2.23) than non-survivors (7.94 ± 3.6; P < 0.001). Using six as cut-off value, JPS had a sensitivity of 85.7%, specificity of 76.3% and diagnostic accuracy of 77.8%.
Discussion
Use of scoring systems for prognostication in intra-abdominal sepsis is a science which is underappreciated and, hence, underutilized. 4 The last couple of decades has seen the publication of many different scoring systems. Basically, each and every system measures the derangement in the physiologic factors representing the severity of illness and function of the major organ systems of the body. Numerical points are given for the severity of the deviation from normal and the outcome of the disease is predicted by the summed weight of all factors. All scoring systems show a strong relation between a high score and high mortality risk. Significant linear relationships have been identified for all combinations of scores, signifying that all the scores, more or less, measure the same events. The utilization of scoring systems enables: stratification of abdominal sepsis according to severity; high-degree prognostication; identification of patients at high risk; patient randomization for clinical trials; comparisons between groups of patients with similar diseases; clinical audit of treatment efficacy; and standards of care. It also objectively supports informed clinical decision-making and is helpful when making cost-benefit decisions.
Surgeons working in sub-optimal conditions in developing countries are hampered by: a lack of the sophisticated and expensive investigative equipment commonly required for these scoring systems; difficulties of objectivity in data collection; and problems of ensuring methodological consistency. Such infrastructural deficiencies constitute academic challenges for developing simple and economical scoring systems for various disorders. 5,6 In the face of these handicaps, we constructed a simple prognostic scoring system for peptic perforation. 3
The steps to be taken in the development of a prognostic scoring system are well known:
7
Establish a precise definition of outcome being predicted; Develop a model of variables that directly influence outcome; Define each predictive variable with good measurement reliability; Collect database with information on predictive variables and patient outcomes; Formulate a predictive instrument that analyzes relationship of variable to the outcome; Validate the instrument.
These steps were followed in the construction of the JPS.
Stratifying the risk with perforation-operation interval while constructing the JPS was considered important, not only because multiple regression analysis proved it significant, but also because the majority of patients reached the hospital late. Our observation of increasing mortality correlating with increasing perforation-operation interval prompted us to keep the range of the scores for perforation-operation interval at 0–4. JPS, when applied to PPP, was shown to be perfectly calibrated and discriminant as the predicted and observed outcome matched. 3
When JPS was applied to TIP patients, it was seen that, stage by stage, they had more morbidity and mortality than PPP patients (Table 4 and Figure 1). The high mortality rates from TIP are partly due to the limited supportive care available in hospitals in developing countries (such as intensive care units, ventilatory support and a lack of metabolic support in the form of total parenteral nutrition) and partly due to disease-related factors such as non-migration of omentum to offer protection which, invariably, causes generalized fecal peritonitis. Up to 100 cm of ileum from the ileo-cecal valve can be affected and severe bleeding can compound the problem. The patient is likely to be anaemic/hypo-proteinaemic and late diagnosis and delay in reaching the hospital are the norm rather than the exceptions in these geographical areas. Non-surgical complications, such as myocarditis, pneumonia, disseminated intravascular coagulation, intestinal hemorrhage and endotoxic shock, when present, worsen the overall prognosis.

Comparison of mortality in peptic perforation peritonitis (PPP; n = 140) and typhoid ileal perforation (TIP; n = 82), as per Jabalpur prognostic score (JPS)
When outcomes were compared between TIP and PPP, two parameters stood out:
Mean perforation-operation interval for survivors being 76.8 h (standard error [SE] =12.8) and for patients who died, 134.2 h (SE = 15.2). Mean perforation-operation interval in TIP patients who died was longer (134.42 h) than PPP patients (99 h). Mortality increased significantly in TIP for each increment of perforation-operation interval (Table 5). In TIP patients, severe respiratory infection was observed in 24 patients, of whom 14 died (P = 0.009); 66% of the patients who died (14/21) suffered from associated severe respiratory infection.
Comparison of morbidity and mortality between perforation-operation interval in peptic perforation peritonitis (PPP; n = 140) and typhoid ileal perforation (TIP; n = 82)
JPS, Jabalpur prognostic score
Our observation in TIP patients suggests that there should be an added weight to these parameters when calculating JPS for TIP. JPS can be easily modified for TIP (JPS-TIP) by doubling the points allotted for perforation-operation interval and allotting six points for severe respiratory illness: JPS-TIP = perforation-operation interval score (×2) + age score + blood pressure score + heart rate score + creatinine score + co-morbidity score + 6 (if severe respiratory infection found present)
After the modification, JPS-TIP for TIP shows good correlation with JPS for PPP (Figure 2).
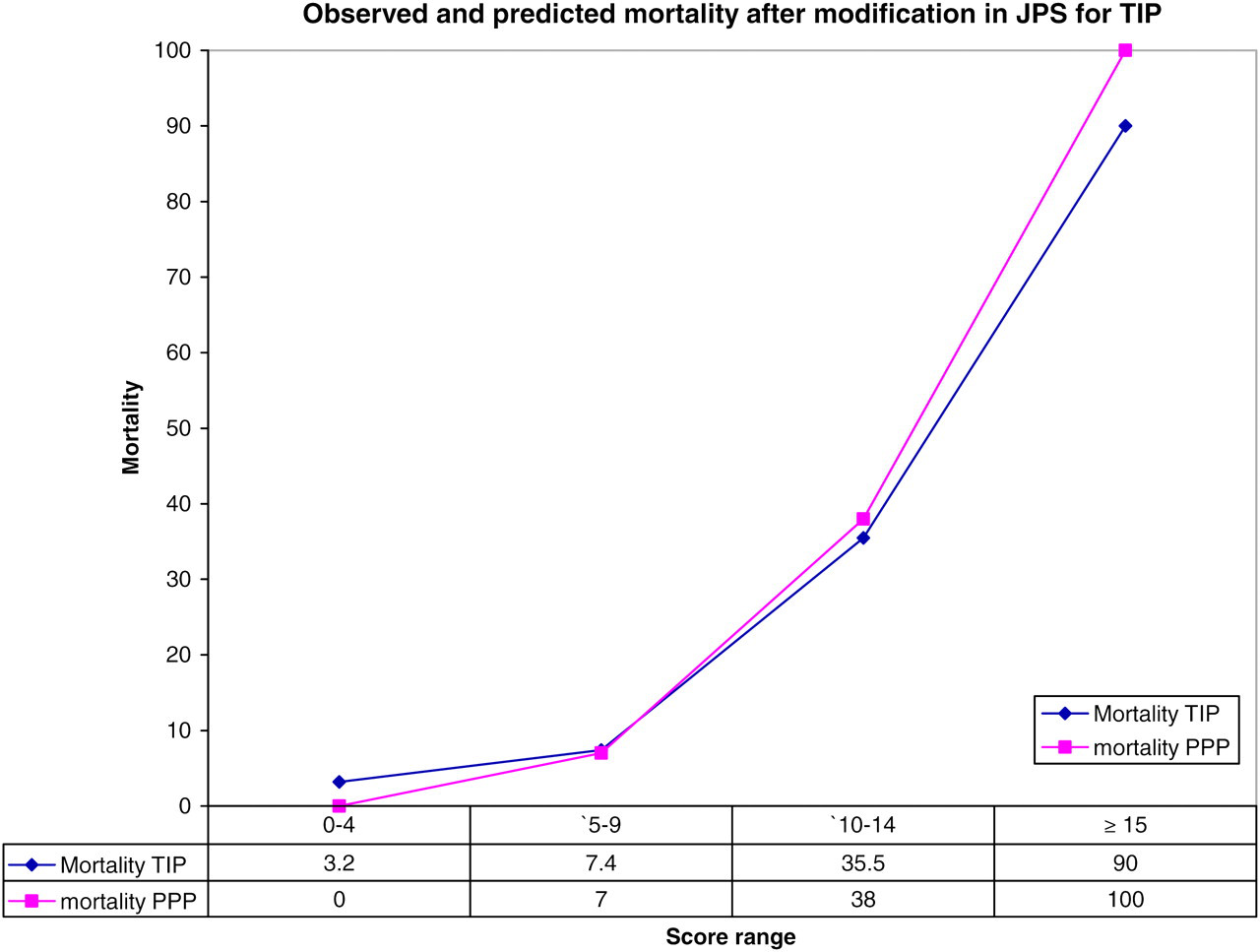
Comparison of mortality in peptic perforation peritonitis (PPP; n = 140, as per Jabalpur prognostic score [JPS]) and typhoid ileal perforation (TIP; n = 82, as per JPS-TIP)
Testing for correlation with the data to which it is being applied is a must for any prognostic scoring system. Geographical variation in the different patient subsets makes such testing and validation mandatory. Since each surgical unit serves a different patient population, each score system must be calibrated in the individual hospital to ensure that the model is applicable to the patient material involved, before the scoring system is accepted as quality standard.
JPS is easier to use than APACHE II or MPI, especially in developing countries, as it incorporates perforation-operation interval – an important prognostic parameter in developing countries, it does not use sophisticated investigations and its simplicity ensures objectivity in data collection and methodological consistency. JPS can be easily applied, with minor modifications (JPS-TIP), for prognostication in TIP. It is quick and easy to use as the number of variables is small. It is suitable for even the smallest of the hospitals in developing countries and requires minimum facilities and all medical personnel can assess each variable objectively. It is user-friendly, the calculation of the risk is easy and it does not require the use of complicated formulae or a calculator.