
Abstract
Summary
The causative factors and ocular complications of Stevens-Johnson syndrome and toxic epidermal necrolysis are reported here. Six out of seven patients developed the syndrome secondary to ingestion of sulphadoxine/pyrimethamine while one developed it as a complication of HAART (highly active antiretroviral therapy). The ocular complications were ankyloblepharon, symblepharon, chronic conjunctivitis, corneal vascularization and conjunctivalization, and blindness. One patient died. A shift to the WHO-recommened artemisin-based combination therapy for the treatment of malaria is advised. Early referral to the ophthalmologist will help to reduce the complications.
Introduction
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are immune complex mediated hypersensitivity disorders which may result in severe morbidity and death (Figure 1).1,2 They may be caused by drugs such as the sulfa group of drugs, anti-TB drugs, viral infections, malignancy and HAART (highly active antiretroviral therapy), especially nevirapine.2,3
Patient with Stevens-Johnson syndrome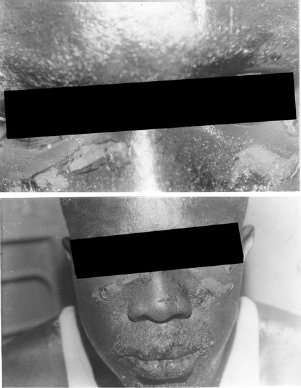
This paper reports on the ocular complications of SJS and TEN presented at the University of Benin Teaching Hospital, Benin City, Nigeria, between June 2006 and September 2007.
Patients and methods
Seven patients (three males and four females) with a diagnosis of erythema multiforme major, SJS or TEN were seen during the study period. The ocular management of these patients included the use of antibiotic and steroid eye drops, tear naturalle, gutt homatropine, chloramphenicol ointment or daily glass rodding to prevent the formation of adhesions or symblepharon. This study was approved by the ethics committee of the hospital.
Results
Six patients developed SJN or TEN secondary to the ingestion of a sulphadoxine/pyrimethamine combination for the treatment of malaria and one developed TEN as a complication of HAART. The age range of the patients was 5 years to 45 years. Two males were HIV-positive. The demographic data and ocular complications of all the patients are shown in Table 1.
The demographic data and ocular complications of patients with Stevens-Johnson syndrome

Case history
Case 1
A 38-year-old woman was seen 11 days after the onset of symptoms with a diagnosis of TEN after the ingestion of sulfadoxine/pyrimethamine. She had generalized blisters, bullae, vesicles and ulcerations. Her visual acuity was hand movement close to the face in the right eye and an ability to count fingers at 3 m in the left eye. There was bilateral ptosis, ankyloblepharon and symblepharon. The conjunctiva was injected and discharging. There were corneal ulcers in both eyes which healed with opacification, vascularization and conjunctivalization. The final visual acuity was hand movement close to the face in the right eye and count finger at 1 m in the left eye.
Case 2
A 5-year-old boy presented with generalized body rash, fever, blisters and ulcers on the skin, lips and eyes after treatment with sulphonamide/pyrimethamine. A diagnosis of TEN and septicaemia was made. He was jointly managed by the paediatricians, ophthalmologists and plastic surgeons. He developed conjunctival adhesions and symblepharon. His packed cell volume was 23% and he was transfused. Despite intensive management he died.
Case 3
A 30-year-old HIV-positive man on HAART (tenofovir, nevirapine, lamivudine) developed TEN. He had a generalized maculopapular rash and mucocutaneous blisters in the periorbital region and the mouth. His visual acuity was 6/6 in each eye. HAART was stopped and he was placed on intravenous steroids and antibiotics. There were no ocular complications.
Discussion
The incidence of ocular complications from SJS and TEN varies with the degree and severity of the systemic disease. 4 Drugs, especially sulphonamides, are responsible for 50% to 60% of cases. 2 In this report six of the seven cases developed erythema multiforme secondary to ingestion of sulfadoxine/pyrimethamine while the seventh patient developed the reaction from HAART. SJS has been reported to be the most common adverse clinical event occurring in HIV patients on HAART. 3
The sulfadoxine/pyrimethamine combination is commonly used in the treatment of malaria in Nigeria. 5 Most of the HIV patients with SJS in a hospital in Malawi developed it secondary to intake of sulphodiaxone/pyrimethamine. 6
Ocular complications in patients in this report were: entropion, trichiasis, symblepharon, ankyloblepharon, dry eyes, punctal stenosis, corneal conjunctivalization, corneal ulcers, opacities and blindness. Two of the patients did not develop any ocular complication because they were referred to the ophthalmologist early. Ocular complications in TEN, which occur in 50% of patients, may be quite extensive and can result in long-term complications including blindness. 1
The management of patients with SJS and TEN involves a multidisciplinary approach. Early referral to the ophthalmologist is important. The inciting drug should be discontinued. Ocular management includes the frequent instillation of tear supplements, topical antibiotics, cycloplegics and glass rodding. The use of topical and systemic steroids in the early stages of the disease helps to reduce the chronic ocular complications. Bandage contact lenses, punctal occlusion, corneal grafts and epithelioplasty have been used. Limbal epithelial stem cell and amniotic membrane grafting are successful in treating the disease. 7
Surgical lysis of symblepharon should be done but the patients in this report refused to undergo this treatment. Medical practitioners should use the World Health Organization artemisinin-based recommendation for treatment of malaria.