
Abstract
Summary
We have previously described a seizure disorder characterized by head nodding (HN). In a prospective study in southern Tanzania, we evaluated 62 patients with HN. Here, we report the patients’ clinical characteristics and those of their seizures, which indicate high seizure frequency, unsatisfactory seizure control, a high burden of cognitive impairment and disease-associated barriers to education.
Introduction
In 1962, LJ-A described several children with attacks of ‘nodding head’ in Mahenge, a village of southern Tanzania.1–3 Interestingly, a progressive disease characterized by head nodding (HN), mental retardation and stunted growth, termed ‘nodding disease’, has been observed in southern Sudan since the mid-1990s. 4 Possible causes have remained obscure.
We recently described the semiology of 62 people with HN in southern Tanzania and suggested a clinical classification. 5 We further conducted electroencephalography, magnetic resonance imaging (MRI) and skin as well as cerebrospinal fluid polymerase chain reaction of Onchocerca volvulus, a filarial worm, whose implication in the genesis of epilepsy has been discussed controversially. 5–7 According to our findings, HN may represent complex partial seizures or atypical absences, a genetic syndrome and/or may be associated with infection of O. volvulus. The relevance of each of the possible causes would have to be explored in further studies. 5
To date, information on HN is still scarce. In our study, we collected details on the clinical presentation of HN seizures, medical and psychiatric history, as well as the sociocultural aspects of people with HN, which may be relevant to the attending physician, in order to further characterize this unexplored seizure disorder.
Methods
Study site and patient recruitment
The study was conducted in 2005 in The Mahenge Epilepsy Clinic, which is situated in the Ulanga district of southern Tanzania. Patients known to suffer from HN seizures were recruited consecutively and underwent interviews via a questionnaire. Physical, neurological and cognitive examination was performed by three neurologists (ES, WM, ASW) and one psychiatrist (LJ-A).
Definitions
HN is defined as a repetitive short loss of neck muscle tone resulting in a nodding of the head, sometimes associated with a short loss of muscle tone of the upper extremities. 5 We classified people with HN seizures as ‘HN only’ or ‘HN plus’, the latter being associated with other types of seizures. 5
As there is no standardized IQ Test for the rural African population with a high rate of illiteracy, cognitive impairment was estimated by level of education, observed behaviour and the ability to follow age-related instructions. In severe cognitive impairment, there was major interference with daily tasks.
Results
Demographics and seizure classification
The average age at the time of interview was 14.9 ± 4.3 years with a 3:2 female preponderance. In 87.1% (54) of all patients HN started between the age of 6 and 15 years. Twenty-eight patients had ‘HN only’, 34 patients suffered from ‘HN plus’ (28 with one and six with two other types of seizure; for further details see Winkler et al. 5 ).
Clinical characteristics of head nodding seizures
The average time from first HN seizure to presentation to the Epilepsy Clinic was 2.2 ± 3.0 years. Interestingly, the time increased when people were suffering from other types of seizure. Patients with ‘HN only’ came after 1.1 ± 1.1 years. Patients with one, and those with two other types of seizure, presented after 2.9 ± 3.7 and 4.4 ± 4.7 years, respectively. The difference between the diagnostic groups was almost significant (Kruskal-Wallis test, P = 0.071).
At the time of the study, all but three patients were on antiepileptic therapy. Before treatment, more than half of the patients (34) had daily HN seizures, 21% (13) had HN seizures 2–3 times/week and 24.2% (15) 1–5 times/month. The average frequency was 22.1 ± 21.7 seizures/month. While the patients were on treatment, there was a significant reduction in seizure frequency (10.9 ± 11.5 seizures/month, t-test, P < 0.001). However, the majority (45.2%; 28) still reported HN seizures 1–5 times/month and a considerable percentage (21.0%; 13) still had daily HN seizures. Forty-eight (77.4%) of the patients had their last HN seizure within a week before the interview.
Clinical details of people with HN
Past medical histories included common diseases such as simple malaria, gastrointestinal and respiratory tract infections. Febrile seizures and meningitis was reported from 12 and three patients, respectively (Table 1). The birth history was unremarkable in all patients. During pregnancy six mothers were unwell: five had simple malaria and one had eclampsia. Fifteen (24.2%) showed abnormal milestones in their childhood and delayed development. In total, 40.3% (25) showed signs of impaired mental capacity – 12 showed severe and 13 slight to moderate cognitive impairment. Of these 25 patients, 15 (60%) had one other type of seizure in addition to HN and this was statistically significant (Fisher's test, P = 0.032, Table 2). The temporal relationship between onset of seizures and mental retardation is also shown in Table 2.
Past medical histories of people with head nodding (HN) sorted by different diagnostic groups
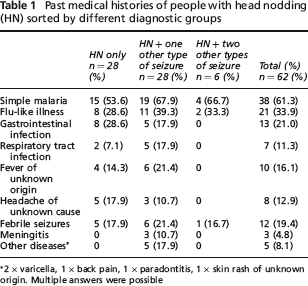
2 × varicella, 1 × back pain, 1 × paradontitis, 1 × skin rash of unknown origin. Multiple answers were possible
Temporal relationship between onset of head nodding seizures and cognitive impairment

Schooling
A total of 35 patients (56.5%) had attended, or were still attending school. At the time of interview, 13 children were still going to school. The highest level achieved was Standard 7 (primary school has 7 years: Standard 1–7). The average grade achieved was 2.4 ± 1.6. In the 21 patients (33.9%) who dropped out of school, epilepsy/HN was by far the most common cause (19; 90.5%). Ten students (28.6%) had already dropped out at Standard 1. Of the present study sample, 27 (43.5%) received no education at all, mainly due to epilepsy and/or cognitive impairment.
Discussion
Our results suggest that HN seizures are extremely frequent, often with daily HN episodes. Treatment on average led to a reduction of seizure frequency by 50%. However, two of 10 people with HN still had daily seizures. Whether poor seizure control in some of the patients is due to the limited choice of antiepileptic drugs (mainly phenobarbitone and phenytoin), non-compliance or other causes will need to be investigated further, ideally in a longitudinal follow-up study, which is currently being planned. Interestingly, the threshold for access to medical care was fairly low in people who had ‘HN only’ but significantly increased when other mainly generalized types of seizures were present. It can be assumed that HN has less of a stigma compared to grand-mal seizures, which clearly represents an advantage for successful treatment of people with HN.
When looking at the past histories of those with HN, two results stand out. Almost 20% of those interviewed remembered febrile seizures, although there was no significant connection between febrile convulsions and hippocampus changes on MRI. 5 Over 40% of those with HN seemed to have cognitive impairment, half of them severely. This is in sharp contrast to 19.4% of a cohort of 371 people with mainly generalized epilepsies recruited from the same Epilepsy Clinic. 8 Most people with HN with impaired mental capacities also had generalized seizures. In terms of temporal relationship, in most patients mental handicap became evident after the HN seizures had started. Cognitive impairment not only has consequences for therapy and prognosis but also bears a sociocultural (schooling) and socioeconomic burden for patients and their families. Causes of the high prevalence of cognitive impairment in people with HN will have to be clarified further and the implications for the choice of antiepileptic treatment considered. Not surprisingly, access to education and standard of performance in school was low in people with HN, with 40% receiving no education at all. In a comparable sample of 321 people with generalized epilepsies from the same Epilepsy Clinic, only 22.4% had never attended school. 8 At the time of the study the nationwide average illiteracy rate was 19.9%. 9
In summary, people with HN seem to be especially vulnerable as a result of frequent seizures, unsatisfactory seizure control, a high burden of cognitive impairment and disease-associated barriers to education. Further research into the above mentioned aspects is definitely needed, together with careful planning of sensitive educational programmes for the patients, their families, medical personnel and teachers alike.
Footnotes
Acknowledgements
We are very grateful to the staff of The Mahenge Epilepsy Clinic as well as to the staff of The Mahenge District Hospital who were very helpful. Our special thanks go to all the patients and their relatives who participated in our study. We are also thankful to the secondary school graduates from Kasita Seminary, Mahenge, who helped with the study. The study was supported by the Savoy Epilepsy Foundation, Quebec, Canada. ASW was supported by the Centre for International Migration (CIM), Frankfurt, Germany. LJ-A, WM and ES contributed equally to the conceptual work of the manuscript.