
Abstract
Summary
A cross-sectional survey of visual impairment (VI) was undertaken in the Enemor district in Southern Ethiopian where five years of trachoma control programme has been implemented using the SAFE (Surgery, Antibiotics, Face washing, Environmental hygiene) strategy. The prevalence of VI (presenting visual acuity in the better eye <6/18) in 451 people above 40 years of age was 22% (CI:17.6 to 27.6) and most of it was accounted for by cataract (67%) and trachoma (13%). Whereas cataract remains a prominent cause, contribution of trachoma among leading causes of VI is declining in communities where SAFE strategy has been implemented.
Introduction
Visual impairment (VI), defined as visual acuity (V/A) <6/18, affects 300,000,000 people worldwide. 1 Cataract and refractive errors account for most of the VI while trachoma remains the leading infectious cause. 1 Trachoma is a chronic bacterial conjunctivitis that results in visual loss from corneal opacity. Blinding trachoma particularly affects communities living in poverty. 2 Approximately 40.6 million people are suffering from active trachoma and 8.2 million might have trichiasis. 3 In Ethiopia alone, VI affects 5.3% of its 73 million people and trachoma accounts for 8.8% of the overall VI. 4
SAFE (Surgery, Antibiotics, Face washing and Environmental hygiene) is the recommended control strategy to achieve Global Elimination of Trachoma by the year 2020 (GET2020). 5 Although the implementation of SAFE is expanding, its impact on trachoma VI impairment remains undetermined. Operational researches provide an alternative source of evidence for policy making and programme monitoring. 6 The aim of this study was to determine the prevalence of VI and to analyse trends in the proportion of trachoma VI in a SAFE programme area in Ethiopia.
Methods
Design and ethics
A population-based cross-sectional survey of VI was conducted in 2006 in the Enemor district of Gurage Zone. The area had a population of 100,000 in 2001 and 110,000 in 2006. Substantial resources have been spent on the implementation of all the components of SAFE in the area. Individuals >40 and household heads were eligible for the study. Ethical approval was obtained from the London School of Hygiene and Tropical Medicine and the local health-care officials. Individuals provided informed consents to participate in the survey.
Sample size and sampling
Sample size was determined based on 20% as the expected prevalence of VI with a precision of ±5%, confidence level (CI) of 95%, cluster effect of 1.5 and 15% contingency. 7 A two-stage random cluster sampling technique was employed to select participants: (1) seventeen clusters were identified from 48 eligible villages using probability proportionate to the size sampling method; and (2) a cluster of 32 households within a village was randomly identified using the ‘compact segment sampling’ method. Two-thirds of household heads were also interviewed on the impact of SAFE in their area.
Data management
Two questionnaires were used to collect data in face-to-face interviews. One ophthalmologist, two nurses and two enumerators conducted the survey. People were tested for vision at 4 m in open daylight using a LogMAR chart. Those with V/A < 6/18 had a further eye examination in order to determine the cause. Individuals with treatable conditions were treated on-site or referred for treatment. Presenting V/A < 6/18 > 3/60 in the better eye was defined as low vision while those with <3/60 were labelled blind. A bilateral corneal scar covering the pupillary margin that appeared in adulthood after years of trichiasis defined trachoma VI. 8 The presence of any lens opacity was taken down as cataract VI after ruling out other causes. The survey data was managed with EPI-data V3 and the analysis was done using EPI-6 statistical software. A comparison of current and baseline proportions was made using 95% CI, considering cluster effect of 1.5. 7
Results
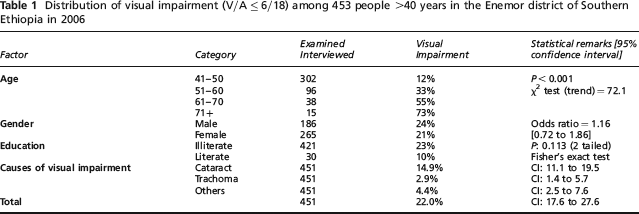
Of the enumerated 473 individuals, 95% were examined. People above 40 years old constituted 17.1% of the population. The prevalence of VI was 22% [CI: 17.6 to 27.6]. The prevalence of blindness and VI in people over 50 was 5.7% and 14%, respectively. The risk of VI was not affected by sex or educational background but significantly increased with rising age. Following cataract (67%), trachoma (13%) caused most of the VI (Table 1).
Distribution of visual impairment (V/A ≤ 6/18) among 453 people >40 years in the Enemor district of Southern Ethiopia in 2006
The prevalence of VI among 2639 people was 20% [18.1–21.9] in the year 2000 in the Gurage zone and in 22% this was caused by trachoma. 7 Compared to these baseline figures, the magnitude of VI remained the same but the proportion of cataract significantly rose by 62%; from 9.2% [7.9–10.7] to 14.9% [11.1–19.5]. The prevalence of trachoma VI declined by 40%, from 4.3% [3.5–5.4] to 2.9% [1.4–5.7], although this was not statistically significant. The actual number of visually impaired people as a result of trachoma declined from 731 in 2000 to 542 in 2006 (Figure 1). Fifty-four per cent of the 371 household heads believed that trachoma VI had been considerably reduced since the introduction of SAFE.
Comparison of the proportion of trachoma visual impairment among people above 40 in the Enemor SAFE programme area of Ethiopia in 2000 (Left, N = 17,000) with findings in 2006 (Right, N = 18,700)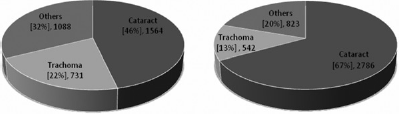
Discussion
The prevalence of trachoma is the ideal indicator when monitoring the impact of SAFE. However, undertaking surveys that require a large sample size is costly for small programmes. Measuring the contribution of trachoma to VI might indicate the overall direction of the effect of SAFE. The burden of VI remained relatively stable in the Enemor area. However, the contribution of trachoma declined while that of cataract increased. Cataract was the leading cause of VI and, as observed elsewhere, increasing age was associated with VI.1,4,9,10
The number of blind people increases with the growth and ageing of populations.1,10 However, the actual number of people with trachoma VI is declining in the Enemor area. This reduction may well have been higher as the specific baseline figure for Enemor is likely to be higher than the zone average and five years might also be an inadequate time period for SAFE to have such a dramatic vivid effect.
The main limitations of the study were its cross-sectional design, the small sample size and the lack of specific baseline data for the intervention area. The association between SAFE and the trachoma VI was difficult to prove without conducting a number of controlled intervention trials. Confounding factors such as socioeconomic status and level of education are likely to alter the effect of SAFE. However, the noticeable drop in trachoma-related VI cases can partly be attributed to SAFE. This observation was reflected by the subjective view of more than half of the community.
Conclusion
Our observations suggest that the contribution of trachoma to VI is declining in communities where the SAFE intervention has been implemented and we therefore recommend that the implementation of SAFE should be continued in Enemor. Long-term controlled studies comparing SAFE areas with non-SAFE areas are required in order to generate more conclusive evidence on the effect of SAFE on trachoma VI.
Declaration of conflict of interest
None of the authors has financial conflict of interest in this study.
The sponsors had no role in the design, implementation or publication of this work.
Footnotes
Acknowledgements
The Association of Physicians of Great Britain and Ireland, ORBIS International, UK, Thomas Spence Dunn Trust and Ophthalmologic Society of Ethiopia covered the financial expenses of this study. We would like to thank the Enemor and Ener District Health Office, Gurage Zone Health Desk and the West Gurage Project office of ORBIS International, Ethiopia, for facilitating the survey.