
Abstract
Summary
Uroflowmetry, urethrocystoscopy and urethrography are either not readily available or the cost is prohibitive for many patients in low-resource countries. This paper examines the use of clinical history in post-urethroplasty follow-up. We retrospectively reviewed the outcome of 54 post-urethroplasty patients. Preoperative diagnostic work-up included simple blood tests and a retrograde urethrography, and postoperatively we did not perform any immediate diagnostic work-up. Follow-up of these patients was done through mobile phone calls and personal contacts. Eighty-nine per cent of our patients reported acceptable voiding over a mean follow-up period of 48.4 months – 79.6% were followed using mobile phone contact. In the majority of the urethral strictures cases, diagnostic work up can be kept to a minimum, thereby reducing cost. Follow-up can be done via phone calls and personal contact in many African countries where compliance is frequently less than encouraging. The spread of mobile phone networks across the continent has been remarkable.
Introduction
Urethral stricture is a very common urological disease and there are a variety of treatment approaches depending on stricture location, length and aetiology.1–7 Across Africa, urethral stricture is a very common disease.8–10 The choice of treatment available in African countries is often determined by: the cost involved in obtaining the treatment; the availability of trained specialists; and access to special instruments. 11 As a result, it is not unusual to see patients suffering from stricture disease who have had suprapubic tube drainage for many months or even years. It is, therefore, very important that simple strategies are developed which minimize the cost of treating urethral stricture, which may enable many needy patients to undergo definitive repair. Monitoring of treatment outcome across Africa is still poor12,13 as many patients do not return to clinics for follow-up, especially if they are not feeling ill. The lack of follow-up is primarily related to the financial cost involved either for recommended postoperative work-up or for transportation to the clinic which often may be far from the patient's locality. Also, there is currently no consensus on the optimal approach to patient management following urethroplasty.14– 17 In recent years, there has been a dramatic increase in the use of cell phones in Africa but, to date, there have been no studies that have evaluated the use of mobile phones and personal contact to assess surgical outcomes in Africa.
Since 2002, we have simplified our protocol for treating urethral strictures using simple blood tests and retrograde urethrography preoperatively and monitoring of a patient's symptoms postoperatively. The purpose of this study is to evaluate the effectiveness of our simplified pre- and postoperative testing programme on patient outcome. Furthermore, we sought to evaluate the use of mobile phones and personal contact to monitor long-term voiding outcomes following stricture repair.
Methods
This study was a retrospective review of a consecutive series of 54 patients with various urethral stricture in various locations treated between July 2002 and October 2007.
Preoperative evaluation included detailed history taking of symptoms that prompted patients to present to us. Laboratory investigation included haemoglobin, urine analysis and creatinine. All our patients had retrograde urethrography as the basic investigation for diagnosing the presence and length of the urethral stricture. However, in two patients the stricture was discovered incidentally in the process of doing a transurethral resection of the prostate for benign prostate hyperplasia. In three patients, in whom the retrograde urethrography did not give adequate information on the proximal aspect of the stricture, we went ahead with performing voiding cystourethrography. In the immediate postoperative period, we did not obtain an imaging study in order to assess the adequacy of stricture repair following catheter removal. After catheter removal all patients had a seven-day course of oral antibiotic. Our criterion for a successful stricture repair was the patient's confirmation that they were able to urinate freely without difficulty.
We had contact addresses for all the patients and mobile phone numbers for those that had mobile phones, or the mobile phone numbers for the friends and relatives of patients who did not have a mobile phone. We also collected the details of members of our hospital staff who knew these patients and could act as a contact for us in order to obtain long-term follow-up information about them. The 45 patients with access to mobile phones were called up at least three times in the first year and at least twice thereafter to check on their condition. For the nine patients who did not have access to mobile phones, we sought information through contacts twice for the first year and at least once thereafter. We checked to confirm that the patients were urinating satisfactorily, that they were happy with their treatment and that they had no problems.
Results
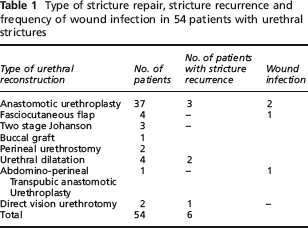
The median age of our patients was 38.5 years (range of 16–80 years). Sexually transmitted infections were the most common cause of urethral stricture in our series. The operations performed, recurrence and wound infection rates are shown in Table 1. There was one case of haematoma that did not resolve spontaneously and which had to be drained. Catheter dislodgment occurred in one patient a few hours after surgery but the catheter was successfully reinserted. The majority of our patients had a stricture located in the bulbous urethra (Table 2) and most of the strictures were between 1–1.9 cm (Table 3).
Type of stricture repair, stricture recurrence and frequency of wound infection in 54 patients with urethral strictures
Location of strictures
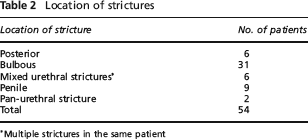
Multiple strictures in the same patient
Length of strictures
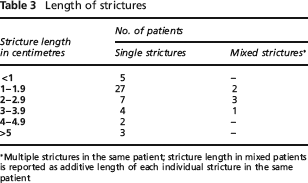
Multiple strictures in the same patient; stricture length in mixed patients is reported as additive length of each individual stricture in the same patient
We were able to obtain long-term follow up via mobile phone calls for 43 of our patients (79.6%) and a further nine were reached by personal contacts, resulting in a combined long-term follow-up rate of 96%. Two patients could no longer be contacted 16 and 21 months after surgery. Their mobile phone numbers were no longer active. We had three recurrences after anastomotic urethroplasty at 1.5 months, 3 months and 8 months (giving a successful surgical outcome of 91.8% for anastomotic urethroplasty). These patients were offered a repeat operation – anastomotic urethroplasty in two and fasciocutaneous flap repair in the other patient. Two patients had recurrences after dilatation and one after direct vision urethrotomy. They then underwent anastomotic urethroplasty and all were fine.
In summary, 48 of the 54 patients had a good outcome and needed no further surgery. All the patients who recurred contacted the main author when they started to notice difficulty with urination. Their complaints were mainly of recurrent poor urine flow and straining to urinate. The patients were invited back to the hospital for control retrograde urethrography that confirmed re-stricturing. The mean follow-up time was 48.4 months (range: 28 to 89 months).
Discussion
In this series, we treated 54 patients with urethral stricture. Our patients urinated well after catheter removal without any diagnostic confirmation of the adequacy of the repair site and the majority remained so on long-term follow-up. Without patients having to come for routine in-hospital check up, we were still able to receive the necessary information on the treatment outcome. Forty-eight of the 54 patients (89%) had a successful repair which compares favourably with other series in which patients underwent intense routine post-repair urethrography and uroflowmetry.
Prior to implementing the simplified protocol for the evaluation and monitoring of urethral strictures described in our report, we had very limited information on the success rate of stricture repair in our centre as many patients simply could not afford the intensive post-repair imaging and compliance with follow-up visits was poor. Maskew et al. 18 identified financial constraint as the leading cause of failure to follow up in their study of patients on antiretroviral treatment for HIV/AIDS. The recent rapid increase of mobile phones in many countries in Africa,19,20 provides an opportunity to use these cell phone contacts to improve medical follow-up and reduce the costs involved. Blake 19 noted that mobile phone subscriber numbers in Africa increased by over 1000% between 1998 and 2003, bringing the total to 51.8 million. We were able to contact directly or indirectly 43 (79.6%) of our patients via a mobile phone.
Our model of follow-up was mainly based on getting patients back to the clinic as soon as they noticed any difficulty with urination. We were able to obtain information about the patients’ wellbeing through phone calls and personal contacts and were thus able to assess their long-term voiding function. In Africa, it is culturally acceptable and appropriate for hospital workers coming from the same village to personally contact patients to verify outcomes. With this combined approach we were able to obtain long-term follow-up results in 96% of our patients. We believe that our mobile phone and personal contact method of long-term patient follow-up was successful and could be applied to other surgical diseases in Africa and other developing countries, thereby providing long-term outcomes where historically long-term data has often been deficient. Furthermore, our streamlined postoperative patient management and follow-up regime could be undertaken in select patients living in remote areas of developing countries where long-term follow-up is logistically difficult and travel is expensive. Our patients expressed their profound gratitude for this mode of follow-up that had saved them the considerable cost of travel.
Cost has always been an inhibiting factor when accessing surgical care in many areas of Africa and the developing countries.21–23 Ogbonna 9 noted that only 31% of the patients with urethral stricture that he studied were able to afford the cost of contrast urethrography. Reducing the number of pre- and postoperative diagnostic procedures and eliminating the expenses of travel for routine follow-up visits can only help to make surgery more affordable to many needy patients. On average our patients spend approximately US $60 for retrograde urethrography, which is equivalent to the monthly income of many inhabitants in our locality. There was no incident of a complication among our patients that occurred as a result of our streamlined approach to post-repair management and patient follow-up.
There were some limitations to our study. We define a successful stricture repair as one for which the patient reports being able to urinate freely without difficulty. This definition is a functional one and does not necessarily correlate with the caliber or diameter of the urethral repair. Arnold has shown that a recurrent stricture may narrow to 10 Fr before it causes difficult urination or reduces the urine flow rate. 24 However, we believe that a functional definition of a successful repair may be more relevant than imaging or uroflowmetry data, in the sense that a revision of a stricture repair is unlikely to be advised for someone who reports acceptable voiding and has a minimal to moderate change in urethral caliber. The real issue is how often are intensive post-repair imaging and uroflowmetry studies helpful and at what cost. How many tests need to be performed following urethral stricture repair in order to improve one patient's long-term outcome? Our study suggests that the economic cost to the patient benefit ratio for routine post-repair follow up studies may be low. It is of interest that other urologists are also suggesting that an assessment of the patient's symptom should be the first step in following patients after urethroplasty. 25 Considering that most urethral strictures recur within the first two years, our relatively long period of follow-up shows that our approach can be used effectively in low-resource countries where cost and compliance with follow-up can be a big issue.
Conclusion
In the majority of urethral stricture cases, pre- and postoperative diagnostic work-up can be kept to a minimum without compromising treatment outcome. Follow-up of patients can be done by phone calls and personal contacts, especially in developing countries where adherence to in-hospital follow-up is often less than encouraging. Mobile phones can play a big role in assessing long-term outcomes due to its rapid and increasing usage by many people in developing countries and, thereby, help to reduce the deficiencies in long-term data from those countries. However, it is very important to instruct patients to return to the clinic immediately if they become symptomatic following stricture repair.
Footnotes
Acknowledgements
The authors would like to thank Dr Gerald Larson of the University of Louisville (Kentucky, USA) for all his comments and suggestions during the preparation of this paper.