
Abstract
Summary
Scrub typhus is a commonly encountered rickettsial disease of the Indian subcontinent. Humans are infected accidentally and the case fatality can be significantly high if the disease is not identified in time. We report nine cases of scrub typhus from the Garhwal region of the newly created north Indian state of Uttarakhand, a region not previously known to harbour the vector. Entomological studies are needed to study the density of the vectorand to institute vector control measures in order to prevent this relatively benign, yet potentially fatal, clinical entity from spiralling into a major public health issue.
Introduction
Scrub typhus is endemic in regions of eastern Asia and the south-western Pacific (Korea to Australia) and from Japan to India and Pakistan. It is estimated that there are about one million cases of this disease each year. 1 This illness is caused by Orientia (formerly Rickettsia) tsutsugamushi, an obligate intracellular Gram-negative bacterium, which was first isolated in 1930. The causative organism is transmitted to human beings by the bite of a larval Leptotrombidium mite (chigger). Human beings usually become infected when they accidentally encroach upon an area of infected chiggers in mainly rural and sub-urban areas. If the diagnosis is delayed, or the patient is not treated with the appropriate antibiotic, there can be serious complications such as renal failure, myocarditis, septic shock, meningoencephalitis and, rarely, acute respiratory distress syndrome. The mortality rate is 7–30%. 2
Although common in the first half of the 20th century in India, there have been few reported cases of the disease since then. There were reports of the disease during the Indo-Pakistan conflicts in 1965 and 1971. In 1990, 11 cases were reported from the North Western part of the country. 3 Six cases from among the troops from the eastern sector and two cases from the northern sectors were reported in 1993.4,5 In the present decade, outbreaks of scrub typhus were validated in southern India in 2003, 6 West Bengal and Shimla in 2005, West Bengal, Manipur and Nagaland in 2006 and Himachal Pradesh in 2007 (data from the National Institute of Communicable Diseases [NICD]).
The newly-formed north Indian state of Uttarakhand, with thick forest cover that could provide a fertile breeding ground for the mite, has not reported a single case of this disease. The authors suspected and diagnosed the disease in nine patients from the Garhwal region who presented with a high grade fever of short duration, anaemia and hepato-splenomegaly with or without hepatic, renal and respiratory failure.
Case profiles
Table 1 summarizes the clinical and demographic profiles of the nine cases. All the patients belonged to the Garhwal region of Uttarakhand and presented over a period of 15–20 days. None had a recent history of travelling to an endemic region. All the patients presented with a fever of 1–2 weeks’ duration and with gastrointestinal complaints, mainly pain and vomiting. Respiratory distress was present in three patients.
Clinical and demographic profiles of patients diagnosed as suffering from scrub typhus
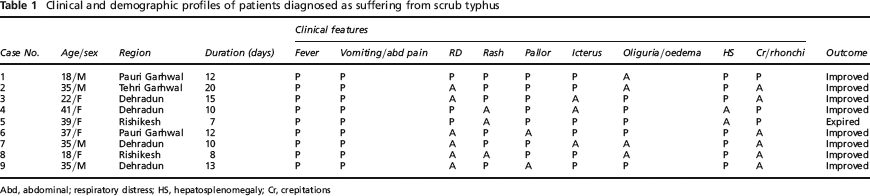
Abd, abdominal; respiratory distress; HS, hepatosplenomegaly; Cr, crepitations
The haematological and biochemical profiles of all these cases are shown in Table 2. Although all cases, except one, demonstrated a dramatic clinical, haematological and biochemical response to doxycycline, the diagnosis was made retrospectively by IgM ELISA using the 56 kDa antigen of the Orientia tsutsugamushi in the sera of the patients at the NCID, New Delhi. The antigen has a proven sensitivity of 86.5% that increases considerably after acute febrile illnesses (namely, falciparum malaria, pulmonary TB), Streptoccocus viridans septicaemia and typhoid fever have been ruled out. 7
Haematological, biochemical and radiological profiles of patients suffering from scrub typhus at presentation
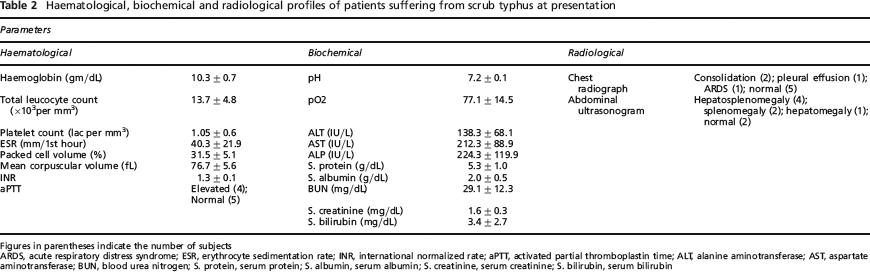
Figures in parentheses indicate the number of subjects ARDS, acute respiratory distress syndrome; ESR, erythrocyte sedimentation rate; INR, international normalized rate; aPTT, activated partial thromboplastin time; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BUN, blood urea nitrogen; S. protein, serum protein; S. albumin, serum albumin; S. creatinine, serum creatinine; S. bilirubin, serum bilirubin
Discussion
The term ‘scrub’ is used because of the type of vegetation (terrain between woods and clearings) that harbours the vector. However, the name is not entirely correct as certain endemic areas can also be sandy and semiarid. As in previous reports,3,6,8 we noted that these cases occurred during the cooler months of September and October. All our cases presented with a fever of short duration, hyperaemia of the skin over the anterior abdominal wall and thighs, subconjunctival haemorrhages and hepato-renal insufficiency. Acute respiratory distress syndrome (ARDS), a rarely reported but serious complication of scrub typhus, was seen in two of our cases. It has been reported in a three-case series from the sub-Himalayan city of Shimla, located at a similar altitude and with a similar climate as the area from which our patients hailed. In India, the rash is not generally seen,4,9 but we observed a hyperaemic macular rash located centrifugally in all our patients. Anaemia is also an uncommon finding in scrub typhus which may be attributed to intravascular/extravascular haemolysis because of the acute illness and hypersplenism.
These infections respond well to antimicrobials like doxycycline and chloramphenicol. 10 However, mortality can be high if the disease is untreated 11 and has been reported as 15% in tertiary care centres when complications have developed. 2,5 All our patients showed a dramatic response to doxycycline and the only mortality observed was in a patient who, at presentation, had severe hepato-renal dysfunction with ARDS.
The distribution of mites can be very patchy as, to support the larvae, they require an environment where the adults have an abundant prey population and through which mammals frequently pass. The local climate must also be one in which the mites do not have to dig too deep for protection as this prevents egg-laying. Scrub typhus is endemic in a large part of India but it had not previously been observed in the north Indian state of Uttarakhand, despite the fact that the climate is one which is suitable for the breeding of the vector. The Garhwal region is hilly with ongoing infrastructural and industrial development conducive to vector breeding. The fact that the rainfall in this season was almost twice the annual average, causing the soil to remain loose, probably led to an increase in number of eggs laid by the mites.
The qualitative IgM ELISA against 56 KDa antigen in the patients’ sera was used by us as it is a rapid and objective test which has been widely reported to accurately test the large numbers of sera often obtained in seroepidemiologic investigations. 12 Other acute illnesses such as malaria, sepsis, enteric fever and TB had been ruled out before these sera were sent for analysis at the NICD, New Delhi.
Our cases presented with multiorgan dysfunction within the first week, with ARDS observed in a few. Health providers should, therefore, be aware of this potentially fatal, yet curable, infectious entity in the eventuality of a larger outbreak of disease. As no vaccine for scrub typhus is available at present, short-term vector reduction using environmental insecticides and vegetation control, or chemoprophylaxis with doxycycline in high-risk groups, should be instituted in the future.