
Abstract
Summary
Seasonal outbreaks of febrile illness with eschar have been occurring in Bishnupur district of Manipur since 2001. The aetiology of these outbreaks was unknown. We investigated a similar outbreak in 2007 in order to confirm the aetiology and identify its risk factors. We identified 38 patients who met the case definition (attack rate: 3.4/1000), including two deaths (case fatality ratio = 5.3%). Half of the female patients had eschar on the perineal area. The clinical picture and Weil-Felix positivity suggested that the outbreak was due to scrub typhus. The disease was more common among individuals who defecated or urinated in the jungle or bushy areas from a squatting position. We recommended educating the community about the common symptoms of the disease, encouraging them to seek early treatment from public health facilities and suggested that they be taught to avoid defecating/urinating from a squatting position in the jungle.
Introduction
Scrub typhus, caused by Orientia tsutsugamushi, is transmitted through the bites of infected trombiculid mites. 1 Humans become infected when they encroach on an area where the mite-rodent cycle is occurring. 2 The disease is characterized by a primary ‘punched out’ skin ulcer (eschar) corresponding to the site of an attached infected mite, regional lymphadenopathy and maculopapular.1–2 In India, scrub typhus outbreaks have been reported from several states, including Tamil Nadu, Himachal Pradesh and Sikkim. 3
Since 2001, seasonal, post-monsoon outbreaks of febrile illness with eschars and high case fatality have been reported in Bishnupur district in Manipur, a northeastern Indian state. Since its aetiology had not been established, the disease was locally known as ‘Khullai-laipha’. During July 2007, a similar outbreak occurred in a municipal area of Bishnupur (n = 11,233). We investigated this outbreak in order to confirm the aetiology and to identify its risk factors.
Materials and Methods
Descriptive epidemiology
Following the report of one death due to Khullai-laipha on 25 July 2007, we established a surveillance in the municipal area where four community health workers, two private practitioners and the district hospital were asked to report the occurrences of any cases of Khullai-laipha. We clinically examined all the identified cases and defined a suspected case of scrub typhus as the occurrence of fever with eschars since May 2007. We collected information on the demographic details, residence and date of onset of the eschar. We collected sera from eight patients and examined them for OXK antibodies using the Weil-Felix test at the Kurseong Sub-divisional Hospital, Darjeeling District, West Bengal. A titre of 51:80 was considered to be positive. 4
Analytical study
We conducted a matched case-control study by including all the identified suspected scrub typhus patients. For each case, we selected four age-, sex- and neighborhood-matched healthy controls. We collected information on their environmental exposure during the previous 21 days.
Data analysis
We described the outbreak by time, place and the individual and conducted a conditional logistic regression analysis in order to identify the risk factors associated with the illness using Epi Info software.
Results and discussion
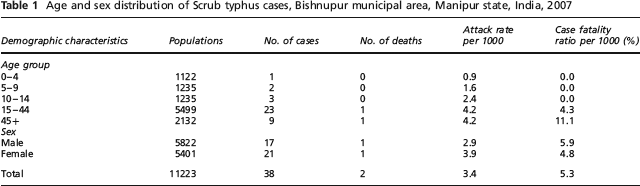
We identified 38 suspected scrub typhus cases which included two deaths (attack rate: 3.4/1000, case fatality rate: 5.3%) (Table 1). Attack rates were higher among females (3.9/1000) and those aged 515 years (4.2/1000). Five sera were positive for Weil-Felix test (titres 1:80–1:320). Twenty-one cases (55%) had eschar on the perineal area, 14 (37%) on head/neck/shoulder or chest and three (8%) on thighs and lower abdomen.
Age and sex distribution of Scrub typhus cases, Bishnupur municipal area, Manipur state, India, 2007
Besides high-grade fever and eschars, the common symptoms among the patients included headache, cough, chest pain, lymphadenopathy, restlessness, respiratory and abdominal discomfort. Cases started appearing from 27 May 2007 and peaked during the 2nd week of July 2007. The last case was reported on 27 September 2007. Eleven patients were treated with doxycycline and seven with azithromycin, while the remaining 27 had received treatment from traditional healers.
On a conditional logistic regression analysis, the odds of developing the disease were significantly higher among individuals who stored firewood in and around their homes (odds ratio [OR] = 32, 95% confidence interval [CI] = 4–265), were involved in vegetable plucking or farming (OR = 56, 95% CI = 5–673), slept or sat on the floor without a mat (OR = 16, 95% CI = 1.3–202) and defecated or urinated in the jungle or bushy areas from a squatting position (OR = 20, 95% CI = 2.3–174).
During the outbreak in Bishnupur, we identified several environmental exposures associated with the development of scrub typhus that are likely to expose an individual to a potential bite from an infected mite. Individuals who defecated or urinated in the jungle or bushy areas were also found to be at increased risk. It is a common practice among women to pass urine in a squatting position. High attack rates among females and more than half of the females having eschar on their perineal area indicate that the practice of defecating/urinating in jungles or bushy areas is associated with the exposure to infected mites. Exposure of the body, including squatting to defecate or urinate, has been identified as a risk factor for scrub typhus in India and elsewhere.4,5
Our investigation had certain limitations. First, we could not demonstrate the causative agent in mites. Second, our case definition included patients with fever and eschars, whereas some patients might present without eschars. Third, the diagnosis was based on the Weil-Felix test, which is not a gold standard test. However, due to the lack of availability of confirmatory tests, the Weil-Felix is considered to be useful, especially when interpreted in the correct clinical context in India. 6 Thus, based on the clinical picture and positivity to the Weil Felix test, we suggest that the outbreak was most probably due to scrub typhus.
Based on our results, we recommend educating the community about the common symptoms of the disease and encouraging them to seek early treatment from the public health facilities and not from traditional healers. One simple and practical measure for the prevention of this disease would be to educate the community, especially the women, to avoid defecation/urination from a squatting position in the jungle or bushy areas. It is also necessary to establish facilities for laboratory diagnosis and initiating a health facility-based surveillance in the district.