
Abstract
Summary
The objective of this study was to compare the efficacy and side-effects of two regimens of vaginal misoprostol for second trimester voluntary medical termination of pregnancy (MTP) according to the MTP Act of India. A randomized trial was conducted in 185 women from January 2007 to September 2008. Women in group 1 were given vaginal misoprostol 400 μg every 6 h for a maximum of four doses. Women in group 2 were given vaginal misoprostol 400 μg every 12 h for a maximum of four doses. Our primary outcome measure was induction abortion interval. Secondary outcome measures were success rate, side-effects and completeness of procedure. Results were calculated applying Fisher's exact test, chi-square test, Z test and calculating the P value using an alpha level of 0.05 for Type I error. The mean induction abortion interval in group 1 (12.59 h) was significantly shorter (P <0.001) than that in the group 2 (16.41h). The percentage of women who achieved successful abortion within 12 h in group 1 (56.52%) was also significantly higher (P = 0.00005) than that in group 2 (25.80%). The incidence of side-effects was comparable and not clinically serious. It is concluded that the regimen of vaginal misoprostol 400 μg every 6 h was more effective than the regimen of misoprostol every 12 h in medical termination of second trimester pregnancy.
Introduction
Safe and legal abortion is considered to be a key intervention for improving women's health and quality of life. 1 In our country a significant number of women practice contraception, but medical termination of pregnancy (MTP) is also used to control family size and birth spacing. 2 As a result, an overwhelming proportion of induced abortions (6.7 million annually – an indirect estimate) take place in India 3 and elective termination of second trimester pregnancy is considered as a commonly performed gynaecological procedure. 4
Although several methods have been tried over the years with varying success, the ideal method for mid-trimester abortion remains elusive, as indicated by the constant search for new methods.4–8 Ethacridine lactate has a long history of use in our country and is recommended for use for mid-trimester MTP. 6 However, its use has certain disadvantages such as a longer instillation abortion interval, a higher failure rate and more chances of incomplete abortion.7,8
Misoprostol, a prostaglandin analogue, is principally used to prevent peptic ulcer disease induced by nonsteroidal antiinflammatory agents. 5 It has been shown to induce second trimester abortion.5,7,8
Our recent study showed that vaginal misoprostol 400 μg every 12 h is a more effective and convenient method than ethacridine lactate instillation for the termination of second trimester pregnancy. 7 Pharmacokinetic studies show that the systemic bioavailability of vaginally administered misoprostol is three times higher than that of orally administered misoprostol. With vaginal administration, peak plasma levels occurred later and were lower, but elevated plasma levels were sustained for at least up to 4 h. 8 Assuming that the pharmacological effect of misoprostol is related to its concentration in the plasma, the results suggest that vaginal administration could be dosed at shorter intervals than 12 h. This regimen may be more effective and still have fewer side-effects.
The aim of our randomized trial was to compare the efficacy and side-effects of 400 μg misoprostol administered intravaginally every 12 h with a regimen of 400 μg misoprostol vaginally every 6 h in second trimester MTP. Our study hypothesis was that, using 400 μg of vaginal misoprostol at 6-h intervals would result in a significant shortening of the induction abortion interval in comparison to 400 μg vaginal misoprostol at 12-h intervals.
Methods
This prospective randomized comparative clinical trial was conducted from January 2007 to September 2008 with 185 women at Nilratan Sircar Medical College Kolkata, India. All participants provided written informed consent before enrollment. Ethics Committee of NRS Medical College approved the protocol and this trial is registered as a Clinical Trial, No. NCT00401440.
Inclusion and exclusion criteria
Women attending the hospital for voluntary mid-trimester MTP, i.e. 12–20 weeks (>84 days to ≤140 days) of pregnancy were eligible for the trial. Women were included in the trial if the termination of pregnancy could be made in accordance with the MTP Act of India. 9 Gestational age was determined from the first day of last menstrual period (LMP) and per abdominal findings. Ultrasonography was done in selected women where LMP and clinical findings did not agree. Medical, gynaecological and obstetric histories were recorded and examined for vital parameters; routine haematological and urine examination were done in all women. We excluded women who had undergone previous uterine surgery or any contraindication of misoprostol use (i.e. unstable cardio pulmonary status, hypersensitivity to prostaglandins) from the trial.
Randomization schedule
Randomization was done using a simple randomization method using a table of random numbers. 10 The schedule was constructed so that the number in each group would be balanced for every 10 women recruited. The group assignments were put into sealed envelopes and the envelopes were opened when the women were recruited by the attending physician – which was the point of randomization. The routes of administration and drug dosage were known.
Treatment schedule
Women assigned to group 1 were given misoprostol 400 μg (two tablets of 200 μg) in the posterior vaginal fornix every 6 h, up to a maximum of four doses. Women in group 2 were given misoprostol 400 μg in the posterior vaginal fornix every 12 h up to a maximum of four doses. Drugs were administered by trainee residents and the women were carefully monitored every 4 h for side-effects during the entire period. The side-effects – including nausea, vomiting, diarrhea and fever (temperature 38°C) – were recorded. The blood pressure, pulse, temperature and frequency of uterine contractions were monitored every 4 h by the residents. A pethidine injection 75 mg was given intramuscularly for pain relief when the women requested a painkiller. After the passage of a fetus, whether or not the placenta was passed, all the women received an intravenous infusion of oxytocin, administered as 10 units in 500 mL of Ringer's solution. The products of gestation (fetus and placenta) were examined to see whether the abortion was complete, but ultrasound examination was not performed. Routine curettage of the uterus was performed under general anaesthesia in all women. If the placenta remained undelivered after 3 h of the expulsion of the fetus, or if significant bleeding was noted, curettage was done as an emergency. If the placenta was expelled and no significant bleeding was noted, routine curettage was done at the earliest convenient time. At the time of curettage, expulsion of any obvious placental tissue was noted. Prophylactic antibiotics of penicillin group were administered following curettage. The amount of blood loss during abortion was assessed clinically. If a woman in either group failed to abort 48 h after initiation of the treatment, she was treated by any method of second trimester MTP according to the discretion of the attending physician. Follow-up of the women was until discharge from hospital.
Outcome measures
Our primary outcome measure was induction abortion interval. Secondary outcome measures were: success rate; side-effects; and completeness of procedure. The induction abortion interval was defined as the time from administration of the first dose of misoprostol to the abortion of fetus. A failure of procedure in both groups was defined as the failed expulsion of the fetus at 48 h or the occurrence of systemic adverse signs and symptoms severe enough to preclude further use of the drug. The completeness of the abortion was defined as the expulsion of both the placenta and the fetus by visual examination and no obvious placental tissue was expelled at the time of the routine uterine curettage. Haemorrhage was defined as an estimated blood loss exceeding 500 mL or the need for a blood transfusion. Fever was defined as a rise of temperature to 38°C or more occurring 24 h or more after pregnancy termination.
Sample size
We aimed to show that 6-hourly applications of vaginal misoprostol would result in a shorter induction abortion interval than 12-hourly applications of misoprostol. Four hours shortening of induction abortion interval was considered of clinical importance. In our previous study mean induction abortion interval using 400 μg vaginal misoprostol for mid-trimester MTP was 15.5 ± 8 h. 7 In order to detect a difference of 4 h using a significance level of 5% and a power of 90%, the number of women needed in each group would be 88. Allowing a 5% undetermined outcome, 186 women needed to be recruited. Recruitment started in January 2007 and continued until September 2008.
Statistical analysis
All data were collected in a pro forma prepared for the study. The data were analysed with Epi Info software and Microsoft Excel software. We did not have a prespecified stopping rule based on the superiority of a regimen before the trial ended. Results were calculated applying Fisher's exact test, chi-square test, Z test and calculating the P value using an alpha level of 0.05 for Type 1 error.
Results
Figure 1 shows the trial profile. The reasons (and some of the women had more than one reason) for non-eligibility were scar in uterus (6, 27.27%) and a gestational age of either <12 (6, 27.27%) weeks or >20 (12, 54.54%) weeks.
Trial profile
Baseline characteristics at trial entry
Of 185 women approached, all provided written consent and were randomized. Of these, 92 women received 6-hourly vaginal misoprostol and another 93 women received 12-hourly vaginal misoprostol. The two groups of women were comparable in respect to age, parity and gestational age reason for MTP and haemoglobin percentage (Table 1).
Baseline characteristics at entry into trial
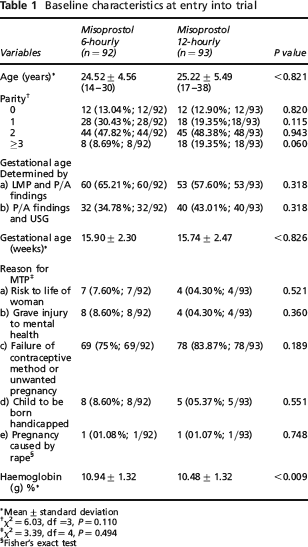
Mean±standard deviation
χ2 = 6.03, df =3, P = 0.110
χ2 = 3.39, df = 4, P = 0.494
Fisher's exact test
Primary outcome
Results for the primary outcome variable and the induction abortion interval are presented in Table 2. As can be seen, a 6-hourly vaginal misoprostol regimen resulted in a shorter induction abortion interval than a 12-hourly vaginal misoprostol regimen. Fifty-two (56.52%, 52/92) women in group 1 had a successful abortion within 12 h in comparison to only 24 (24; 25.80%; 24/93) women in group 2. Thus, a greater number of women in group 1 had an abortion within 12 h (Table 2).
Induction abortion interval
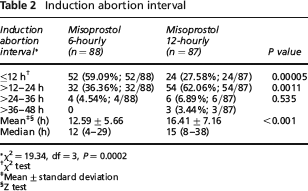
χ2 = 19.34, df = 3, P = 0.0002
χ2 test
Mean±standard deviation
Z test
Secondary outcomes
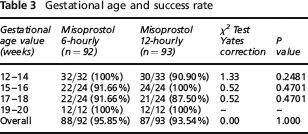
Eighty-eight (88/92; 95.65%) of the 92 women in group 1 and 87 (93.54%; 87/93) women in group 2 had successful abortions within 48 h. The success rate of abortion according to gestational age was comparable (Table 3). All four women who had unsuccessful abortions in Group 1 received extra amniotic ethacridine lactate (EAEL) and had a successful abortion within 18–30 h following EAEL instillation. Of the six women in group 2 who had failure, two received a repeat dose of misoprostol after one day, two received EAEL, one received PGF2α injection and one had a hysterotomy. All these women had successful abortions within a variable period of 6–48 h.
Gestational age and success rate
Side-effects and other secondary outcomes are shown in Table 4. There was no significant difference in the rate of complete abortion among the groups and subsequent curettage revealed no obvious placental tissue in these women. The average time taken for curettage was comparable (6.72 ± 2.91 min in group 1 versus 6.26 ± 3.72 min in group 2, P < 0.531). The incidence of side-effects did not differ between groups and were not clinically serious. None of the women received blood transfusions. The mean dose of misoprostol needed was 1008 ± 179.4 μg in group 1 and 800 ± 184 μg in group 2 (P < 0.001).
Side-effects and other secondary outcomes
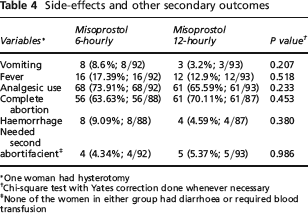
One woman had hysterotomy
Chi-square test with Yates correction done whenever necessary
None of the women in either group had diarrhoea or required blood transfusion
Discussion
There are a number of advantages of using misoprostol instead of other methods for termination of pregnancy in second trimester. Misoprostol is less expensive, does not require refrigerated transport or storage facilities and can be given vaginally, orally or in combination in different dosages.5,8 Several studies have evaluated the use of misoprostol for induction of abortion in second trimester. The optimal regimen has not been determined. Studies have used doses ranging from 200 to 800 μgm at intervals ranging from 3 to 12 h.5,7,8 Doses of 600 μg and 800 μg have shown comparable successful abortion rates but are associated with high rates of fever, diarrhoea, nausea and vomiting. 8
In our previous study we found a high success rate (95%) with minimal side-effects when vaginal misoprostol was used in 12-hourly intervals with a maximum of four doses. 7 Our present trial also showed both 6-hourly and 12-hourly vaginal misoprostol resulted in comparable and high success rate (95% versus 93%, P = 1.000) but induction abortion interval (12.59 h versus 16.41 h, P < 0.001) was shorter in 6-hourly vaginal misoprostol regimen than 12-hourly vaginal misoprostol regimen.
Agarwal and Chaturvedi 11 administered 200 μg of misoprostol vaginally every 12 hours and 80.5% women had an abortion within 24 h. Biswas et al. 12 used 600 μg misoprostol vaginally followed by 400 μg 8 hourly until the expulsion of products or up to 48 h and the success rate was 92% with a mean induction abortion interval of 13.94 h. 12 Edwards and Sims 13 compared two regimens of vaginal misoprostol, one low dose (200 μg every 12 h) and one high dose (400 μg every 6 h), for second trimester pregnancy termination at 13–27 weeks. They found that a high dose regimen resulted in more abortions (98% versus 84%; P = 0.014) and shorter induction abortion intervals (13.25 versus 22.5 h, P = 0.001) without any greater side-effects.
Success rate and induction abortion intervals are major aspects of clinical importance in second trimester MTP. Our study was designed to detect the difference of induction abortion interval between the women receiving 6-hourly vaginal misoprostol and 12-hourly vaginal misoprostol. Results show not only that a 6-hourly regimen results in a shorter induction abortion interval but also that a higher number of women in the 6-hourly group had an abortion within 12 h compared to the 12-hourly regimen (59.09% versus 27.58%, P = 0.00005). From this clinical perspective, a 6-hourly regimen seems to be more effective than a 12-hourly regimen.
The trial reveals that both 6-hourly and 12-hourly regimens result in comparable side-effects. The complete abortion rate was also comparable. We performed a check curettage in all women because, in a significant number of women (33% in our previous study 7 ), vaginal misoprostol use results in an incomplete abortion and our follow-up was only up to the time of discharge from hospital.
Our trial is the first randomized study that has compared two different intervals of application of vaginal misoprostol using the same dose and via the same route for the induction of abortion in second trimester MTP in India. The sample size was large enough to detect a clinically significant shortening of induction of the abortion interval. Our results provide reliable evidence on the use of vaginal misoprostol for the induction of abortion in second trimester MTP and contribute to the available information about its efficacy and safety.
Our trial has included women with all different types of indication of second trimester MTP in a wide age range and parity as per the MTP Act of India. Unlike other studies conducted in western countries, we did not include women with a dead fetus or a premature rupture of membranes. 13 None of the woman refused to participate in the trial. Our results have external validity and are applicable to the general obstetric population requiring MTP.
Concerns remain about the potential for uterine rupture, especially when misoprostol is used in women with a previous caesarean delivery. 5 Therefore, we excluded women with a previous caesarean delivery from participation in the trial. However, as the caesarean section rate is on the rise, further well designed studies are needed for a safe and effective method of mid-trimester MTP in post-caesarean pregnancy.
Footnotes
Acknowledgements
We are grateful to all the women who took part in the trial and the doctors, nurses, trainees and other staff of our hospital, as without their collaboration this study would not have been possible. We are also grateful to Mr Asit Baran Chakraborty, Lecturer in Statistics and Demography, Post Partum Unit, NRS Medical College, Kolkata, for the statistical analysis and interpretation of the results.