
Abstract
This is a practical laboratory overview of current detection methods for malaria parasites, suitable for use in developing countries.
Introduction
Early detection and effective treatment of malaria will shorten its duration and prevent the development of complications and the great majority of deaths from malaria.
Historically, the diagnosis of malaria has involved the microscopic visualization and identification of malaria parasites on thick and thin blood films. The careful examination of a well-prepared and well-stained set of films remains, to this day, the ‘gold standard’ for the diagnosis of malaria.
However, in many developing countries, health-care facilities and funding at a local level are frequently inadequate. Essentials, such as working microscopes and well-trained staff, are often in short supply.
When laboratory facilities are available, the path to accurate diagnosis is fraught with pitfalls. Due to financial constraints, microscope slides are usually cleaned and recycled and, thus, may have plant contaminants, such as pollen grains, on the surface. Scratches and other physical imperfections may also hinder accurate microscopy. Stains kept out on the bench will eventually harbour a large population of contaminating microorganisms. As a result, a variety of artefacts (platelets, pollen grains etc.) are frequently mistaken for malaria parasites (Figure 1).
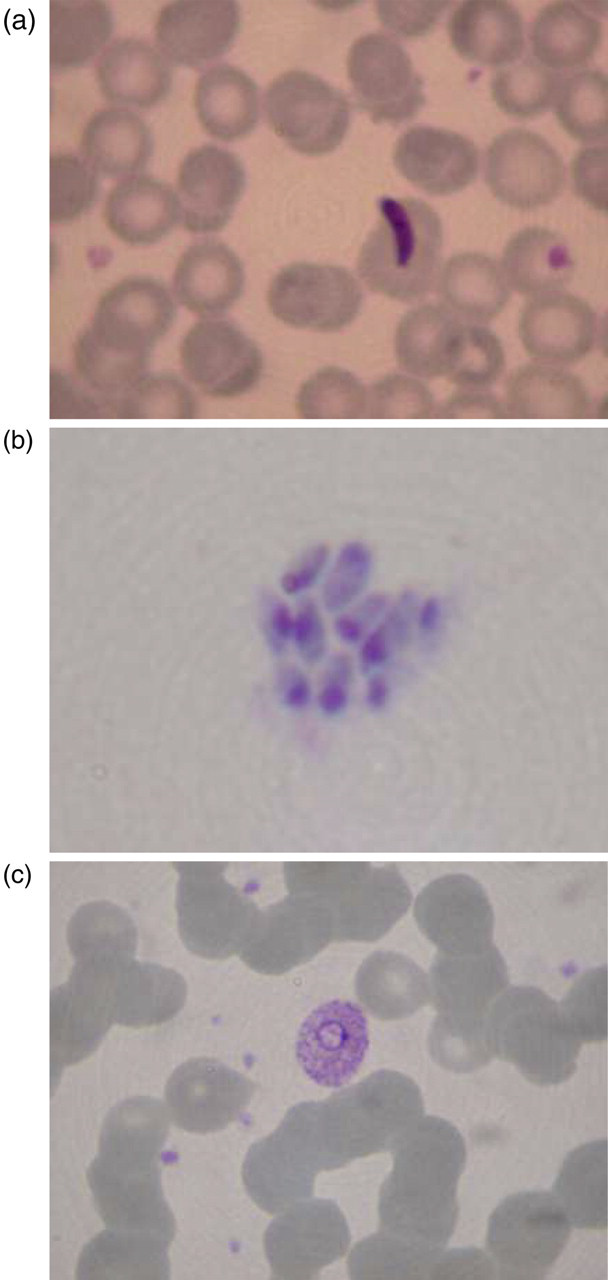
Artefacts mistaken for malaria parasites. (a) Algae; (b) platelets; (c) pollen grains
What can you do to produce good films?
Reserve new/nearly new slides for blood films; Change stains weekly if finances allow; Keeping staining jars covered and refrigerated overnight will prolong the life of the stain; Store slides correctly; If slides need to be left on the bench overnight, store them in a covered container: flies love organic material; Use the very best quality stain that finances allow; Giemsa and Leishman's are commonly used stains. Unscrupulous manufacturers/distributors frequently dilute stock stain: beware of any cheap offers. Check that the bottle seal is intact – if it is broken you should reject the bottle.
Alternative diagnostic methods
Rapid diagnostic tests (RDTs) may offer the possibility of extending the availability of a malaria diagnosis to people in remote areas where microscopy may not be possible. However, there are a myriad of problems that need to be addressed at the local level before embracing the RDT as the salvation to all problems.
The following essential points have been condensed from the following publications:
Cost
Can you afford it? Manufacturers have never pretended that these tests are cheap. The cost of the RDT varies from test to test and from country to country. Whatever test is proposed, budgeting provision needs to take into account the expense of shipping, storage, quality assurance testing and staff training
Sensitivity and specificity
These values are difficult to assess from the published literature and are likely to be influenced by storage conditions and user expertise. Good quality assurance procedures, which should be adhered to by all users, are essential.
Storage
Exposure to extreme temperatures is a major contributor to the poor performance of a RDT. High heat and humidity can rapidly degrade RDTs. It is recommended that only RDT kits which are individually packaged in moisture-proof envelopes should be purchased. Storage, at central and final destinations, must conform with the manufacturer's specifications. Out-of-date tests must be discarded.
Interpretation
The experience and level of training of staff can influence the validity of the tests. Instructions for RDT preparation and interpretation should be clear, concise and in local languages.
Remember:
A negative test result does not always exclude malaria: there may be insufficient parasites present; The RDT may have been damaged; The RDT that is in use may not detect all species of malaria parasites; A positive result does not always signify that the patient has malaria; The antigen may sometimes persist after the parasites have died; In patients with high levels of immunity, the presence of malaria parasites may not necessarily be the cause of their illness.
Quality assurance
Many manufacturers include an internal validity check as part of the RDT operation system itself (Figure 2). However, this is rendered useless if the preparation and storage of the test does not comply with the manufacturers' recommendations.

Quality assurance – internal validity check of the RDT operation system
Conclusion
The World Health Organization state that health workers using RDTs should be trained, assessed and systematically monitored on the preparation and interpretation of the tests.
Clinical confidence and reliance is dependent on meaningful and accurate results. Reliance on a poorly used and maintained diagnostic tool such as a RDT will inevitably result in failures of malaria case management, misdiagnosis and loss of credibility.