
Abstract
Many herbomineral preparations are currently being used as therapeutic remedies for common ailments. Commonly known cardiotoxic herbs are Aconitum ferox (aconite), Areca catechu (betel nut), Thevetia peruviana (yellow oleander) and Cleistanus collinus (oduvan). Herbs mixed with lead, copper and/or mercury are known to be highly toxic. They produce cardiac arrhythmias, mainly ventricular ectopics, ventricular tachycardia and various degrees of arterioventricular (AV) blocks. We report 12 such successive cases where the patients developed vague feelings of discomfort, dizziness, chest discomfort and ventricular arrhythmias following herbal drug ingestion which warranted the immediate discontinuation of the drug. Three of the patients died. This paper emphasizes the risk of unsupervised use of herbomineral preparations by patients who believe that the remedies are always ‘safe’ and the urgent necessity for the pharmacognostic identification of the constituent herbs, their toxicological studies, uniform nomenclature, authenticity and standardization of plants and their parts before advocating them for therapeutic use.
Introduction
There has been a renewed interest in the therapeutic use of herbal drugs. Medicinal plants have been used in all cultures for thousands of years. 1 These drugs are administered for common ailments as well as for specific conditions such as hypertension, coronary artery disease, diabetes and neuropsychiatric disorders, etc. 2 According to the World Health Organization (WHO), 80% of the population of developing countries rely on them as a primary source of health care. Apart from being cheaper and easily available, the general belief that these drugs are comparatively ‘safe’ makes them locally popular. We recently had 12 patents over a period of two years who developed serious cardiotoxicity following the use of herbal preparations. As this has wider therapeutic and policy implications, we believe that it is prudent to report these cases for the wider sharing of our experience.
Case series
A total of 12 patients were admitted after developing symptoms such as palpitations and vague discomfort within 4-6 h of the ingestion of a ‘crude drug’ (Table 1). In all cases, a history of drug intake, denial of any potential co-ingestions and temporal relation between the ingestion of herbomineral preparations and the onset of symptoms were taken as proof that the herbomineral preparations were the underlying cause of the symptoms. They had variable presenting manifestations including hypotension, ventricular arrhythmias and atrioventricular (AV) blocks. Echocardiographic assessment was done in only four cases (cases 3, 5, 11 and 12). No regional wall motion abnormality was noted in any of the cases.
Salient features of the cases with herbomineral drug cardiotoxicity
AV, arterioventricular; CHB, complete heart block; CHF, congestive heart failure; F, female; LBBB, left bundle branch block; M, male; VPC, ventricular premature contraction; VT, ventricular tachycardia
Unfortunately, most such cases presented without any prescription or a sample of a formulation. In most cases, therefore, the complete characterization of the agent was not possible. In only seven of the 12 cases were we able to identify the culprit drug.
In two cases the culprit identified was Withania somnifera. The first case was a 60-year-old man who presented with ventricular tachycardia after taking Withania somnifera (vernacular, aswagandha). He presented in a state of shock but eventually recovered. Another was of a 55-year-old man who also presented with ventricular tachycardia.
Two patients presented with cardiotoxicity resulting from use of Asparagus abscendens (vernacular, safed moslee). The first, a 25-year-old man, had taken a combination of Asparagus abscendens (safed moslee), Asparagus racemosus (vernacular, shatavari), and Glycyrrhiza glabra (vernacular, mulatthi) and had come to us suffering from ventricular tachycardia and shock. The second, a 35-year-old man, presented with ventricular tachycardia and, later, ventricular bigemini. A 50-year-old man presented with dizziness and palpitations which occurred after the intake of aconite (vernacular, bikh). He had hypokalaemia. In spite of his receiving cardioversion, the ventricular tachycardia proved fatal. One patient presented with ventricular tachycardia resulting from Areca and ‘Yograj Guggulu’ (containing 26 different herbs in guggulu resin [Commiphora mukul]). Both improved with the cessation of drug.
Another young girl presented with an alleged history of ingestion of an unknown herbal powder for acne and pain in the abdomen. She developed numbness and loss of power in all four limbs within 15 min of its ingestion followed by vague feelings of illness, nausea and vomiting. Investigations revealed hypokalaemia (serum potassium 2.8 mEq/dL). Electrocardiogram (ECG) revealed polymorphic ventricular ectopics and changes suggesting hypokalaemia. The ECG returned to normal after potassium replacement and the discontinuation of the offending drug.
Of the 12 patients in the present series, two had hypokalaemia and one had hyperkalaemia. In one case, the hypokalaemia was associated with use of aconite. Three patients died. Their deaths were caused by aconite in one case and a mixture of Asparagus abscendens, Asparagus racemosus and Glycyrrhiza glabra in another. The main ECG findings were ventricular premature beats and ventricular tachycardia (Figure 1).
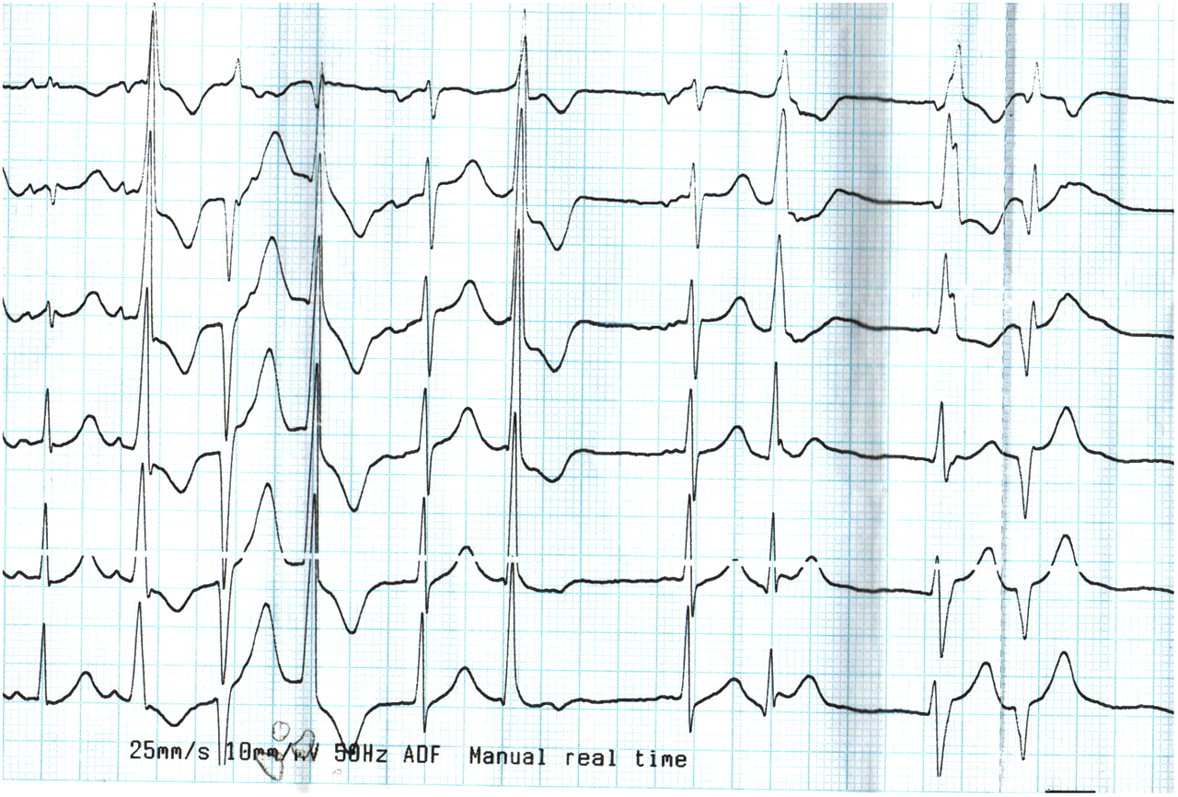
The development of polymorphic ventricular premature contractions in the chest leads (V1-V6) following the ingestion of an unidentified herbomineral preparation for ‘cough’
Discussion
In our series the cardiac toxicity mainly manifested as ventricular arrhythmias. Few of the known cardiotoxic herbs which produce arrhythmia are: Aconitum ferox (aconite); 3 Areca catechu (betel nut); 4 Thevetia nerifolia (yellow oleander); 5 and Cleistanus collinus (oduvan). 6 The active constituent responsible for producing cardiac toxicity has been worked out in aconite, betel nut and yellow oleander toxicity. Aconite has a direct effect on myocardium and adrenals producing release of catecholamines. 3 It is a potent neurotoxin that blocks tetrodotoxin-sensitive sodium channels and block inactivation leading to early and late after-depolarizations but without hyperkalaemia. Areca catechu, another commonly used herb, contains an alkaloid arecoline which produces ventricular arrhythmia: recently, it has also been found to be diabetogenic. 4 Yellow oleander (Thevetia peruviana) possesses a glycoside which produces cardiac arrhythmia simulating digoxin toxicity. 5 Another plant remedy (oduvan [Cleistanus collinus]), primarily used for arthritis-like conditions, has been reported to produce serious urinary potassium loss leading to hypokalaemia and cardiac arrhythmia. 6 Asparagus abscendens, A. racemosus and Withania somnifera may cause bradycardia and hypotension. 7, 8
While it is easy to suspect cardiac toxicity if one knows about the offending herbal drug, often there is no authentic information available. This was the situation for seven of 12 cases in our series. This emphasizes the fact that the development of symptoms such as vague feelings of illness, dizziness and chest discomfort following herbal drug ingestion warrants the immediate discontinuation of such drugs, a close monitoring of blood pressure and cardiac rhythm, an echocardiographic assessment and prompt treatment of the accompanying arrhythmia.
The fact that we could not obtain the actual constituents of these remedies because the facilities for are not readily available in real life clinical practice is of immense concern. Apart from this, other limitations of our report are the lack of objective proof that the patient was using a listed product, other potential co-ingestions (i.e. other medications being used), the sole reliance on history and clinical findings and an absence of the digoxin levels. It was not known whether they were purely herbal preparations or compound formulations which also contained some heavy metals.
Conclusions
In spite of these limitations, this study emphasizes the necessity to be cautious of unsupervised use of herbomineral preparations in the belief that they are always ‘safe’ and the need to control their use so that they are available only in standardized formulations by prescriptions issued by a trained medical professional.