
Abstract
Although the extent of the unmet need for surgeries is well-known, little is known about the surgery performed in district hospitals in sub-Saharan Africa. We review five years of utilization of theatre services at the Kintampo Hospital in rural Ghana. The source of data was the theatre logbook and other hospital records for the period 2005–2009. During this time, 1391 surgeries were performed in the theatre. This approximates a rate of 250/100,000 population. Fifty-two percent were performed in patients aged 18–35 years. The most frequently performed surgeries were: caesarean sections (46%); hernia repair (41%); and other laparotomies (10%). The major indications were cephalopelvic disproportion, right inguinal hernia and typhoid perforation, respectively. Typhoid perforation was the main indication for surgery in children aged less than 10 years. The potential for an expansion of the scope of services should be explored in order to improve access to essential surgery for this population.
Introduction
A fundamental condition for the attainment of health for all and equity in the provision of health services is that all patients should be able to reasonably access basic health care. Access to essential surgery is a basic part of any modern health delivery system. However, the wealthiest third of the global population receives 75% of the world's total number of surgical procedures and the poorest third receive only 4%. 1 Conservative estimates put the overall disease burden associated with surgical conditions in sub-Saharan Africa at 38 disability-adjusted life years (DALYS) lost per 1000 population. This estimate is the highest in the world. 2,3
The primary focus of efforts to address the problem of unmet surgical needs in sub-Saharan Africa is on building capacity at district hospitals and similar first-level referral facilities. 4 As international agencies and local policy-makers consider providing support for the expansion of surgical services in sub-Saharan Africa, accurate data on the current scope of services at district hospitals will be needed to guide decision-making. Currently, such data is either limited or missing altogether. As a result, evidence of the response of the health system to the surgical needs in sub-Saharan Africa is largely anecdotal. 4,5
Ghana is a low-income West African country with an estimated per capita income of US$700 (according to the World Bank Report, 2005). The structure of the country's health delivery system is modelled along the district health-care concept lines. An essential prerequisite of the system is to strengthen the capacity at the district and sub-district levels. The smallest unit of facility care within the system is the health centre at the sub-district level. This facility is expected to offer preventive and curative services, including basic essential obstetric care (EOC). It is usually managed by medical assistants (the equivalent of physician assistants) with the support of nurse midwives, community health officers and health assistants.
The district hospital is the next level up. It serves as the first-level referral facility and is usually situated in the district capital. District hospitals are expected to offer an expanded range of services. The most defining feature is the presence of a medical doctor and the availability of theatre facilities to enable surgery to be performed. District hospitals are expected to offer comprehensive EOC services that include EOC, surgery anaesthesia and blood transfusion. The capacity of district hospitals in Ghana to meet these expectations vary according to availability of equipment and personnel with the requisite surgical skills. 6
The provision of improved theatre facilities at district hospitals is a major priority of the Ghana Health Service (GHS) and, therefore, the service is receiving support from both local and international agencies in order to improve the surgical infrastructure in district hospitals across the country. It is the expectation of policy-makers in Ghana that improvement in surgical services at the district level would make life-saving surgical interventions available to as many in the population as possible. It will also reduce the congestion in regional and teaching hospitals.
The extent to which surgery performed at district hospitals in Ghana is fulfilling these objectives is unknown. Very little information exists on the scope of surgical procedures performed at district hospitals, the extent to which they fulfil the needs of the communities in which they are located and the potential for expanding the scope of procedures performed.
Study setting
The Kintampo Municipal Hospital (KMH) is located in the Kintampo North district of the Brong Ahafo region of Ghana. The municipality defines the exact geographical centre of Ghana and is a major transit point for commuters between the north and south of the country. The district covers a land area of 5108 km 2 and has an estimated population of 110,052. It is home to a large migrant population from the underserved north of the country. Most parts of the district are essentially rural, except for the Kintampo town which is of sub-urban character and recently attained the status of a municipality.
The KMH was established in 1994 and is the only first-level referral facility in the district. Services offered include general in- and outpatient consultations, emergencies, antenatal and child welfare clinics. Specialized dental and eye care services are also offered. The hospital has dedicated inpatient facilities for children, maternal cases and general adult care. The closest second-level referral facility is located 134 km to the south.
The KMH theatre was constructed in 2000. However, due to the lack of personnel, it was not possible to use it until 2003. In the period prior to the establishment of the theatre, all cases requiring surgical intervention were referred to the first-level referral facility of the adjoining district. Although this facility is only 47 km away, the road to the facility was in such a deplorable condition that the journey took well over an hour.
Effective use of the theatre in Kintampo began in 2005. To date, it remains the only facility for major surgical procedures in the district. This paper describes the types of surgery, the indications and the conditions under which the procedures were performed in the theatre from 2005–2009.
Methodology
The main source of data for this review was the logbook kept at the theatre of the hospital. It is used to record information about all surgical procedures undertaken. Supplementary data was obtained from a review of other hospital and administrative records. All data covering the five-year period from 2005 to 2009 were extracted and double-entered into the computer using EPI-INFO (version 3.5.1). The two datasets were compared and validated. Discrepancies were resolved by referring to the original recording in the logbook. The analysis was largely descriptive, with emphasis on related issues of current public health interest.
Information generated after the preliminary analysis of the data was used to develop a short self-administered questionnaire, which was completed by all the medical officers and staff who worked in the theatre over the period of review. Approval for the conduct of the study was obtained from the regional health directorate and administration of the hospital.
Results
A total of 1391 surgeries were performed in the theatre over the five-year period which approximates a mean rate of 250/100,000 population. The highest number (407) was performed in 2008 and the least (138) performed in 2005. The number performed at the hospital increased at an average rate of 76 per year. However, between 2006 and 2007 the number of operations increased by over 100% (from 144 to 317; Figure 1) Staff at the theatre attributed this to the posting of a second medical officer to the hospital in 2006.
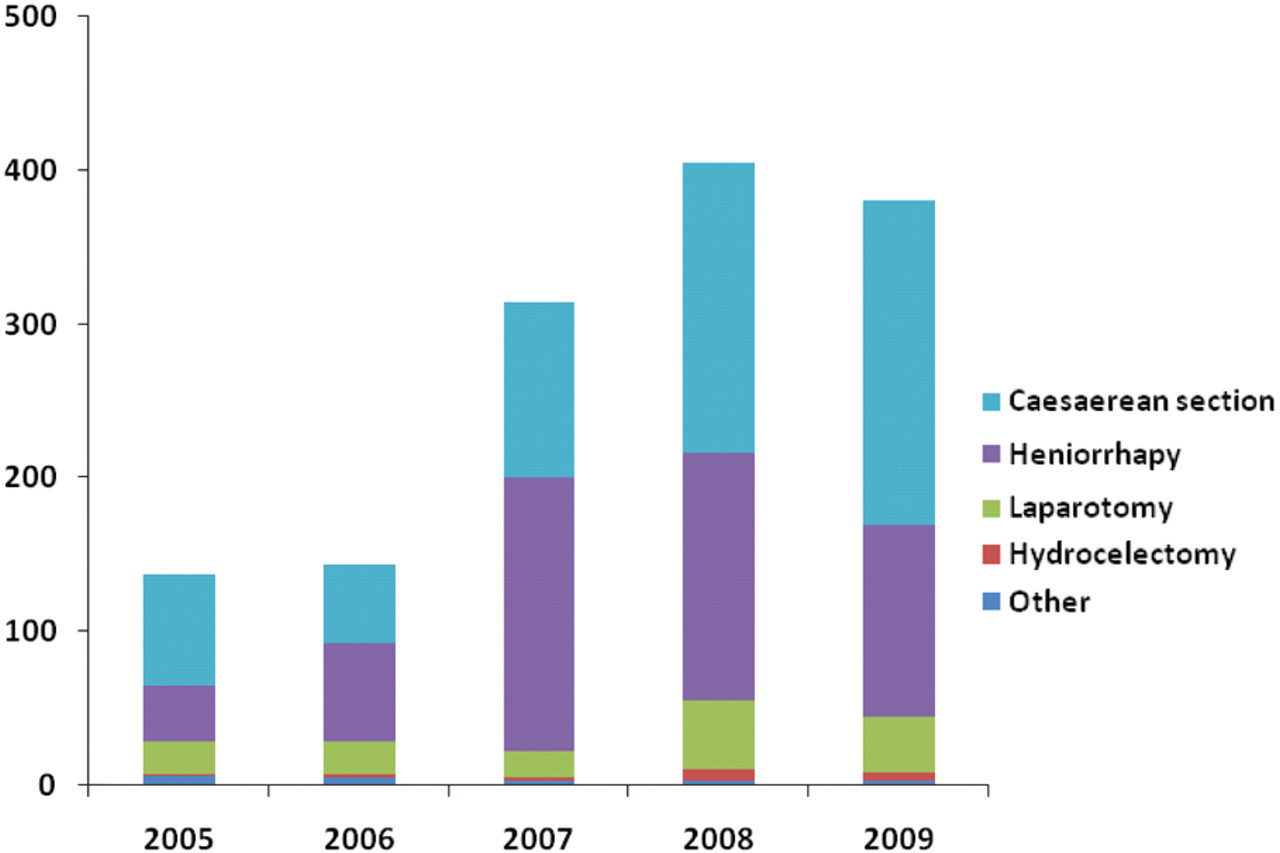
Distribution of the types of surgeries performed per year
More surgery was performed on female patients (61%). This was largely due to the number of caesarean sections performed. The mean age was 30 years (standard deviation = 12 years) and 42 years (standard deviation = 22 years) for females and males, respectively. Overall, 52% of the surgery was performed in patients aged between 18 and 35: 4% in patients aged less than 10 years and 10% in patients aged over 65. The three most frequently performed surgeries were for caesarean section, hernia repair (herniorrhaphy) and laparotomy (Figure 2). The major indications for each of these were cephalopelvic disproportion, right inguinal hernia and typhoid perforation, respectively (Table 1). The number of caesarean sections performed put the rate of caesarean sections at 3.6% of the expected annual number of deliveries in the district. As a proportion of the annual total deliveries in the facility, the caesarean section rates were 7.3% (in 2005), 6.3% (2006), 13.6% (2007), 16.6% (2008) and 13.9% (2009).
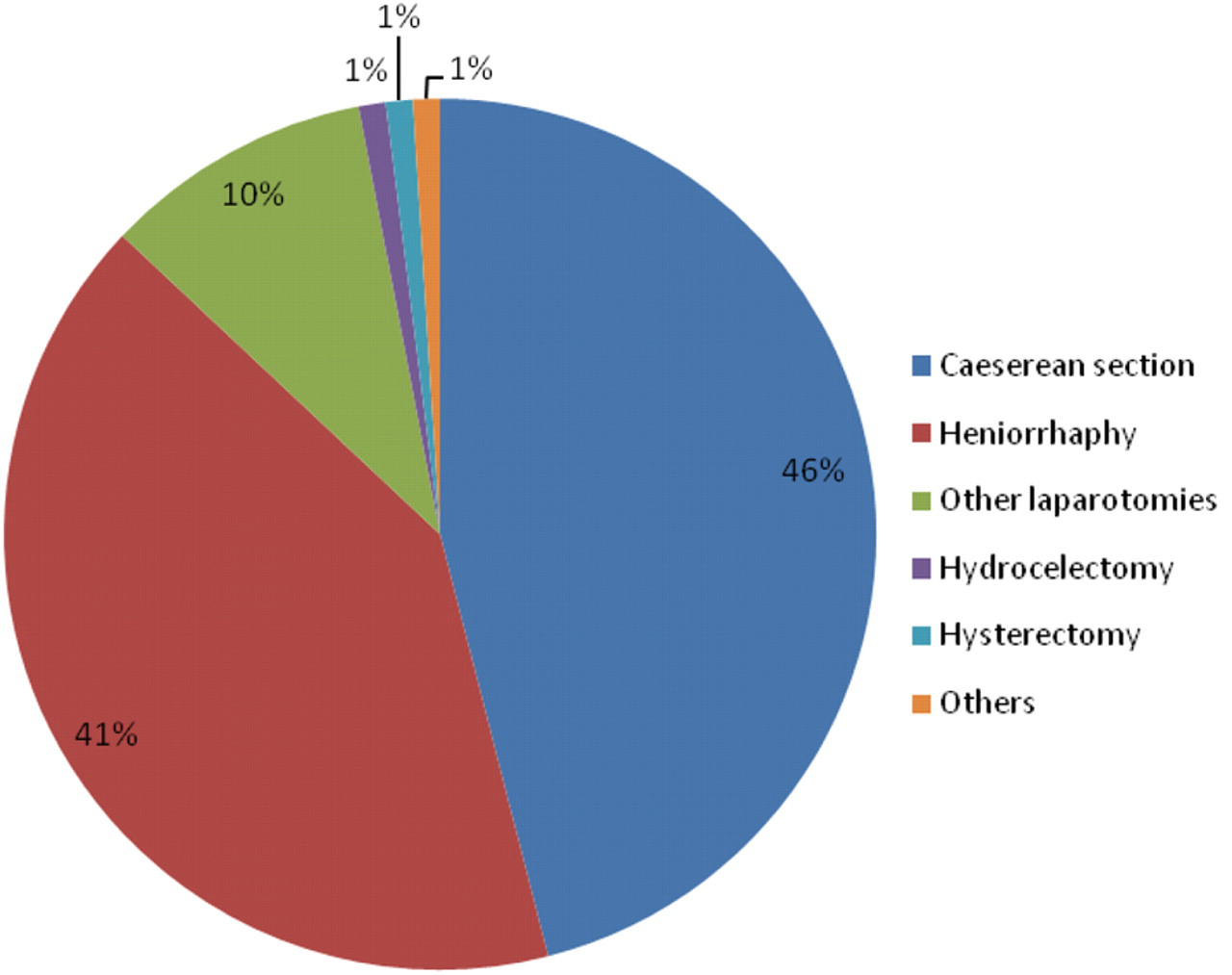
Distribution of types of surgery performed (n = 1391)
Major indications for the three main surgeries performed
In children aged less than 10 years, herniorrhaphy and laparotomy were the two main types of operation performed. Typhoid perforation (3.6% of all cases) was the major indication for laparotomy in children less than 10 years old. It was also in this age group that the highest number of typhoid perforations was observed. Seventy percent of the surgery performed on patients aged 18–35 years were caesarean sections. Herniorrhaphy (94%) was the main procedure performed for patients aged over 65. There were no cases of dilatation and curettage recorded in the logbook.
Most of the surgery (caesarean sections and herniorrhaphy) was performed under spinal anaesthesia, administered by two qualified nurse anaesthetists and one ‘on-the-job’ trained nurse anaesthetist.
Record-keeping
Record-keeping at the theatre was a fully manual activity. A review of records at the theatre showed up considerable inadequacies in the record-keeping. Entries were often illegible, incomplete and/or inconsistent. About 25% of the residential addresses of patients were not entered as required and, in some cases, the sex of patients was either not entered or inconsistent with the name of the patient. In such cases, references had to be made to other hospital records in order to resolve the inconsistencies. The manual approach to record-keeping made the compilation of the summary records tedious. No systematic review of the data had been undertaken over the period in which the theatre had been functioning. The medical officer was the only theatre staff who had received training and had regular access to a computer. None of the other theatre staff had received training in either data management or information technology.
Perception of theatre staff
The theatre staff was unanimous about the positive contribution that the use of the theatre had made to health delivery in the district. They particularly mentioned the opportunity it offered for intervention in obstetric emergencies. It was perceived that the availability of the theatre had contributed to a reduction in maternal mortality in the district. The availability of the resuscitation equipment and the autoclave machine had also assisted emergency care and infection control in the hospital.
On the other hand, the staff were dissatisfied with the inadequate equipment that led to extreme modes of improvisation and also with the lack of training opportunities. They bemoaned their inability to attend to cases of injury, uterine fibroids, haemorrhoids and benign prostatic hypertrophy (BPH). They mentioned that these conditions were prevalent in the community and indicated that the inability of the theatre to attend to such cases constituted a significant disservice to the community. They suggested that a programme be instituted to enable the hospital to invite specialist surgeons and anaesthetists at scheduled times to perform some of these operations and at the same time, offer on-the-job training for staff.
A combination of religious persuasion, uncertainty regarding the position of the law and the lack of a minor theatre were among reasons advanced to explain why cases of dilatation and curettage were hardly ever performed in the theatre. According to the staff, this contributed to exposing women to the unsafe abortion practices of quacks in the communities.
Cost was also mentioned as a factor that hindered access to the surgical services at the hospital. It was explained that, under Ghana's National Health Insurance Scheme (NHIS), very few surgical procedures (including caesarean section) were covered. Thus, the hospital is compelled to recoup its operating cost from patients who undergo procedures that were not covered under the NHIS. The staff perceived that patients found these costs to be too high and that they therefore tended to either stay away or resorted to using traditional remedies.
Discussion
The optimal rate of surgery in sub-Saharan Africa (SSA) is unknown and population-based data on the burden of surgical disease in SSA are urgently needed in order to make it possible to estimate the level of unmet need for essential surgery. Nevertheless, the rate of 250/100,000 population found in this study further confirmed the problem of unmet surgical need seen in similar low-income settings. It compares with an average of 295 across low-income countries and 11,110 in high-income countries.
The findings of this study contrast with those of Lavy et al. 7 who, in 2003, reviewed surgical operations in district hospitals in Malawi and found dilatation and curettage to be the most commonly-performed procedure. Among the procedures performed at the Kintampo Hospital, dilatation and curettage was among the least-performed. The lack of access contributes to making women vulnerable to private practitioners whose high charges effectively precluded access for a substantial proportion of women in the area. The situation has recently been described by Hill et al., 2010. 8
Although, at the KMH, caesarean sections constituted 41% of cases, the combination of caesarean section and dilatation and curettage comprised 37% of cases in Malawi. Just as in KMH, however, the Malawian study found caesarean sections to be among the highest number of cases performed (next to dilatation and curettage). Similar findings were made in studies from Tanzania and Uganda, suggesting that the provision of surgical services in district hospitals constituted an important intervention for ensuring access to comprehensive essential obstetric services in the rural areas of low-income countries. It remains debatable, however, whether the current rate of caesarean section meets the actual need. Until a comprehensive community-based assessment of the need for caesarean sections is conducted, it will be difficult to make conclusive comments on the adequacy of the caesarean sections performed at district hospitals. However, the population caesarean section rate of 3.6 is below the minimum estimate of 5% endorsed by the World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) in 1996. Rates below 5% are considered to be associated with high maternal mortality rates. 9,10
Currently, the scope of surgical procedures that medical officers at district hospital are allowed to perform is not prescribed. To a large extent, it depends on the availability of facilities and the ‘dare-to-perform’ attitude of the practitioners when they are confronted with conditions that present them with very few options. It is also determined by the enthusiasm of the practitioners to learn (in most cases, informally and ‘on-the-job’) additional surgical procedures.
If practitioners are to be motivated to sustain the enthusiasm to learn and acquire more skills in order to expand the scope of procedures performed at district hospitals, then it is important for their efforts to be professionally recognized. There should be mechanisms for appropriate regulation and quality assurance. The institution of a professionally-recognized postgraduate programme in general rural surgery in Ghana and other low-income settings is long overdue. A recent study in Ghana identified a shortage of adequately trained medical personnel as the greatest barrier to improving surgical care in district hospitals in Ghana. 6,11
Rural facilities, such as the Kintampo Hospital, offer the ideal opportunity to harness the opportunity that medical information technology provides for the transfer of knowledge and skills across different settings. Health practitioners in rural areas in low-income countries are usually sole managers of their facilities and are unable to move out of their areas of work for long periods of time. Telemedicine and other innovative distance-learning methods provided from sister facilities should be explored.
In order to overcome the problem of the shortage of medical officers, some low-income countries have offered training and permitted mid-level practitioners (MLP) to perform surgery at the district level. The concept is yet to be formally adopted in Ghana, although undocumented reports suggest that MLPs are engaged in offering surgical services in district and sub-district facilities that lack medical officers. When the concept comes to be formally adopted, Ghana could benefit from the favourable experiences reported from countries such as Mozambique, Tanzania and Malawi where the use of MLPs has been extensively described. 4 In Mozambique, surgically trained nurses and medical assistants perform over 90% of all obstetric surgery. 12,13
One limitation of this review is that it fails to capture a true estimation of surgical needs at the district level. This is because patients in need of procedures that are not performed at the hospital either fail to present themselves at the facility or go directly to second- and tertiary-level facilities. To date, no population-based studies on the need for surgical procedures in the sub-Saharan context have been conducted. A comprehensive needs assessment is required. The findings of such an assessment could be used to define the scope of surgery that can be expected at the district levels and also to guide the development of the professionally-recognized programme mentioned earlier.
In order to improve the record-keeping at the theatre, it is important for the logbooks to be reviewed regularly. Benchmarks of completeness, legibility and consistency need to be set to enable the performance to be evaluated periodically. A data analysis and staff feedback mechanism needs to be instituted in order to motivate staff to appreciate the value of proper record-keeping and to show how it ultimately becomes an indispensable tool for generating the evidence needed to back advocacy for improved infrastructure and services. Given the rate of increase in the number of patients, serious consideration should be given to the use of computers and the application of information technology.
The drive towards a health-systems approach for delivering health-care interventions in Africa opens up an opportunity to redress the long-standing neglect in the provision of surgical services. 5 The dearth of data and information on the utilization of theatre services in rural low-income settings is a challenge. Defining what currently exists and how it could be improved upon are essential initial steps.
Footnotes
Acknowledgements
We would like to acknowledge the contribution and support of other staff of the hospital, particularly those who supported and worked in the theatre during the review period. We should also like to acknowledge the assistance offered to the hospital by the chiefs and people of the Kintampo municipality.