
Abstract
Cardiopathies are common in tropical regions and echocardiography could be of substantial value. However, it is difficult to practice. We suggest simple techniques with conventional instruments that are available in many rural hospitals, and describe the most common echocardiographic procedures and findings that can be undertaken with short training by non-cardiologist physicians.
Introduction
Cardiopathies are common in tropical regions and account for a significant number of hospital visits, hospital admissions and overall mortality. 1
Complicated hypertension with left ventricular hypertrophy (LVH), dilated cardiomyopathy, and rheumatic and post-rheumatic valvular diseases are still common and are a frequent cause of morbidity and hospital admission, 2–6 suggesting that the benefits of echocardiography could be substantial.
Unfortunately, echocardiography is seldom available in the rural areas of developing countries.
We show how to obtain important information with a simple ultrasound scanner and minimal training. In our hospital we trained a physician and obtained good results within a few weeks.
Echocardiography for non-cardiologists
Normal ultrasound scanners are generally equipped with cardiologic software which allows some cardiac measurements for an abdominal probe.
The patient should lie on the left flank with the left arm above the head. Set the instrument to the maximal ultrasound frequency. It is advisable to use lower frequencies when the quality of the images is poor.
The first window is located along the left parasternal line from the second to the fourth intercostals spaces. Point the probe reference towards the right shoulder. In this position it is possible to: measure the antero-posterior diameter of the left atrium (LA) at the end of the atrial diastole (<4 cm); the septum thickness; the left ventricle (LV) posterior wall and internal diameter at the end of diastole at the level of the apex of mitral cusps; examine mitral and aortic valves and the first part of aorta (Figure 1); and to check for anterior (upper part of the screen) or posterior (lower part of the screen) pericardial effusion.
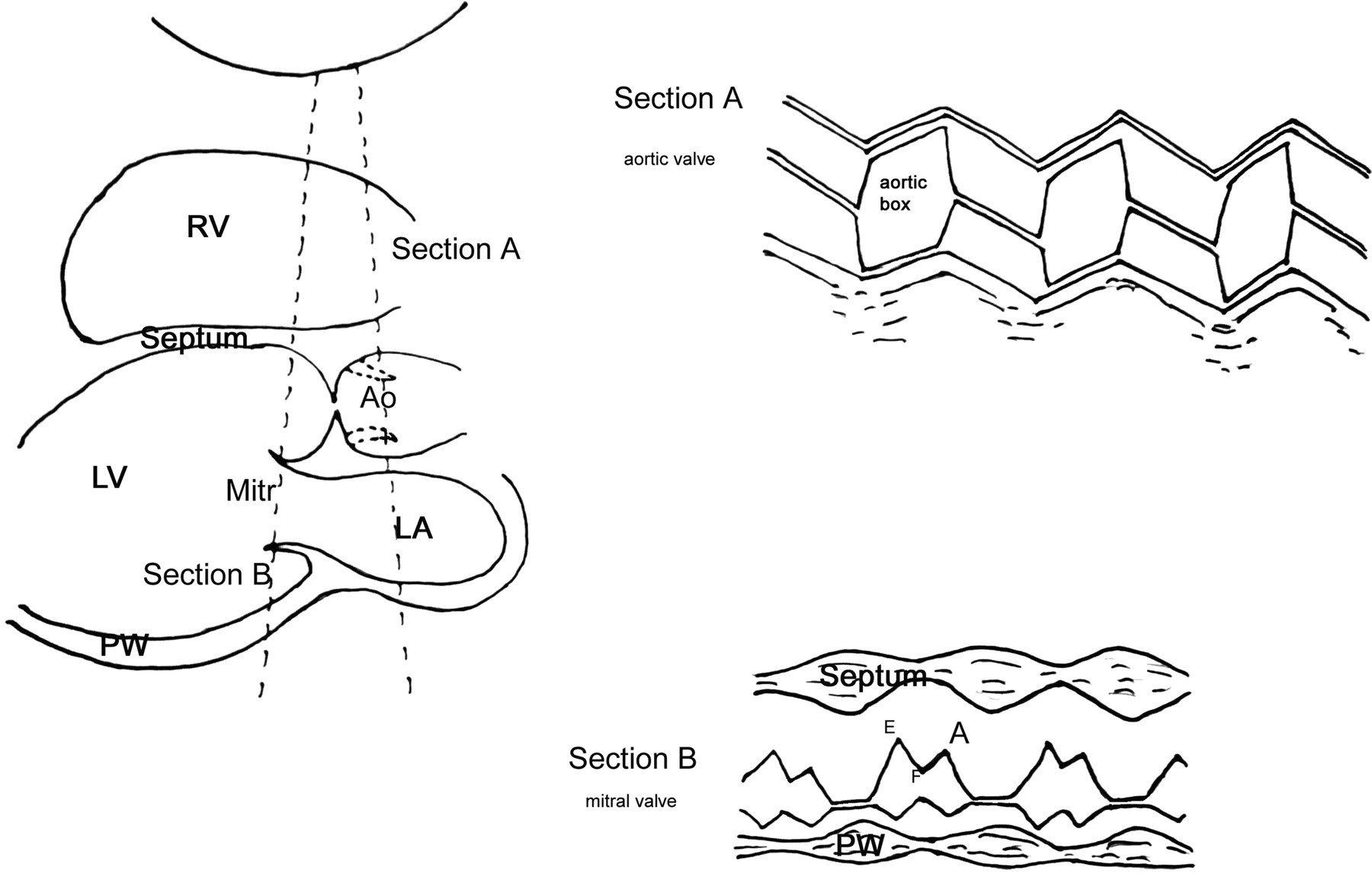
Schematic representation of a long axis left parasternal projection bi-dimensional image, on the left side, and an M-mode image located on the aortic valve (section A upper right side of the figure), and on the mitral valve (section B lower right side of the figure). Mitr, mitral valve; Ao, aortic root and valve; RV, right ventricle; septum, interventricular septum; LV, left ventricle; PW, posterior left ventricular wall; LA, left atrium
Then set the instrument for both bi-dimensional and mono-dimensional (M-mode) scans at the same time. Move the reference line so that it reaches both cusps of the mitral valve (try to obtain images perpendicular to the ultrasound direction) and then pass to the M-mode setting (Figure 1, Section B). In this position you can evaluate the movements of anterior and posterior mitral cusps, normally in an M-shape with two peaks (E and A) and a nadir between peaks called the F point. It is possible to measure the EF segment descending slope in order to find indirect signs of mitral stenosis; the instrument usually provides software to calculate the speed of the anterior cusp from the EF slope. Next, move the reference line to cross the white line that intermittently appears in the middle of the aortic root, above the emergence of anterior mitral cusp. This line appears when the cusps of the aortic valve close together during ventricular diastole (Figure 1, Section A). In this position, in the M-mode setting, it is possible to measure the maximal width between aortic cusps (called the aortic box) and the width of the aortic bulb.
Then move the probe to the apex of the heart, rotating the probe reference to the back, under the left shoulder of the patient (Figure 2). Usually, the instruments can freeze two different images in different times. When the sections of the mitral cusps appear, freeze the images of the end diastole and end systole. Measure the area, and the long and short axis of LV in order to calculate the volumes and the ejection fraction (normally >50%). The LA and the right atrium (RA) can be measured again during atrial diastole. Pericardial effusion can also be measured.
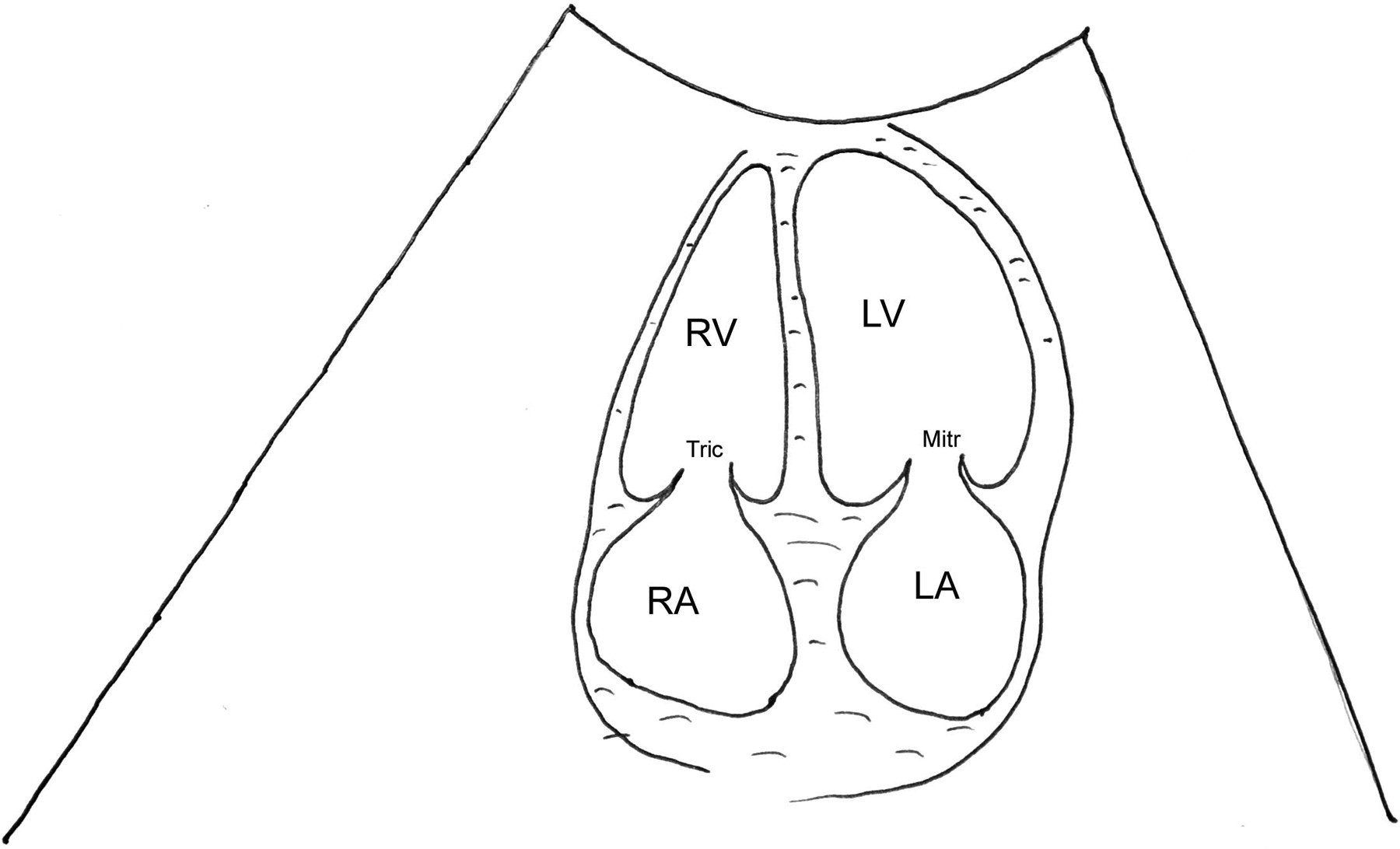
Schematic representation of the apical four chambers’ normal image: RV, right ventricle; LV, left ventricle; Tric, tricuspid valve; Mitr, mitral valve; RA, right atrium; LA, left atrium
Next, move the probe in a sub-costal position under the xyphoid process and the reference towards the left side of the patient. In this position it is usually possible to assess again the presence of pericardial effusion and liver congestion, by observing the intra-hepatic collapse during inspiration.
Pathological findings
Mitral valve disease can be suspected when the LA antero-posterior diameter is increased; mitral stenosis is diagnosed if the EF slope is decreased to less than 70–80 cm/s. Severe mitral stenosis shows an anterior movement of the posterior cusp, a severely reduced EF slope and increased thickness. Mitral regurgitation is difficult to find in the absence of a Doppler scan but can be suspected in the case of atrial dilation with a normal EF slope.
Aortic stenosis is less easy to recognize but can be suspected when: the aortic box is reduced, especially to under 10 mm or less than 70% of aortic diameter; cusps are thickened; and in the presence of LVH.
The diagnosis of aortic regurgitation is more difficult and seldom reliable.
Tricuspidal stenosis appears similar to mitralic stenosis while indirect signs of tricuspidal regurgitation can be suspected in the case of RA dilation and liver congestion.
LVH, concentric or excentric, is recognizable when one or both of the septal and posterior walls exceed 1.1 cm in thickness.
A clinical diagnosis of congestive heart failure can be confirmed and investigated with echocardiography and a determination of ejection fraction with congestion of the intra-hepatic veins. Pericardial effusion appears as an anechogenic (black) space around the heart. It is important to consider signs of tamponade (diastolic collapse of the right chambers), for which urgent pericardiocentesis is needed.
Echocardiography in children
Normal ranges of the measurements change with body surface area or weight. 7 Septal defects are visible only when severe. Most echocardiographic alterations are LVH, pericardial effusion and Fallot's tetralogy, characterized by an aortic root overriding the septum.
Conclusions
Simple echocardiographic evaluation is possible even in a rural hospital equipped with standard ultrasound devices and is able to provide useful information in order to manage most severe cardiac diseases and complications.