
Abstract
Salmonellosis is a common infection in systemic lupus erythematosus patients. The present study reports on two such cases of Salmonella typhimurium septic arthritis among the 102 patients seen during a four-year period.
Introduction
Septic arthritis is a rare consequence of salmonella bacteraemia noted in <1% of cases reported in the literature in patients with an underlying disease such as sickle cell disease or systemic lupus erythematosus (SLE). 1,2 Patients with SLE have an increased incidence of bacterial infections due to hypocomplementaemia, phagocyte defect, cellular defect and use of immunosuppressants and cytotoxic medications as therapy. 3 The infections most commonly involve the lungs, skin and genitourinary tract. 4 From a total of 102 SLE-positive cases seen during four years (2005–2009), 89.2% (91/102) were women and the median age was 28.5 years. We encountered three patients with bone infections, one of whom had osteo-myelitis of the tibia caused by S. aureus while the other two had septic arthritis of the hip joint caused by Salmonella typhimurium. We report these two cases along with their clinical presentation, contributory laboratory findings, disease activity, treatment and outcome.
Case history
Case 1
A 21-year-old woman on steroid therapy, who had been diagnosed with SLE three weeks earlier, was admitted complaining of three days of painful and restricted movements of the right hip. The initial X-ray pelvis and ultra sonogram of the right hip was normal but magnetic resonance imaging revealed an early osteonecrosis of the femoral head in the anterosuperior aspect with 180° involvement without any cortical collapse and with an effusion in the joint space (Figure 1). The C-reactive protein (CRP) level was 147 mg/L on admission. An arthroscopic lavage of the right hip was done and about 20mL of frankly purulent synovial fluid was aspirated and sent for culture and sensitivity testing. Concurrent blood cultures were also sent. She was started on amikacin and ceftriaxone pending the culture reports. Both the cultures grew S. typhimurium which was sensitive to all the routine antibiotics. Amikacin was discontinued and ceftriaxone was continued for one week and she was discharged on oral ciprofloxacin for four weeks. She was lost to follow up after two months.
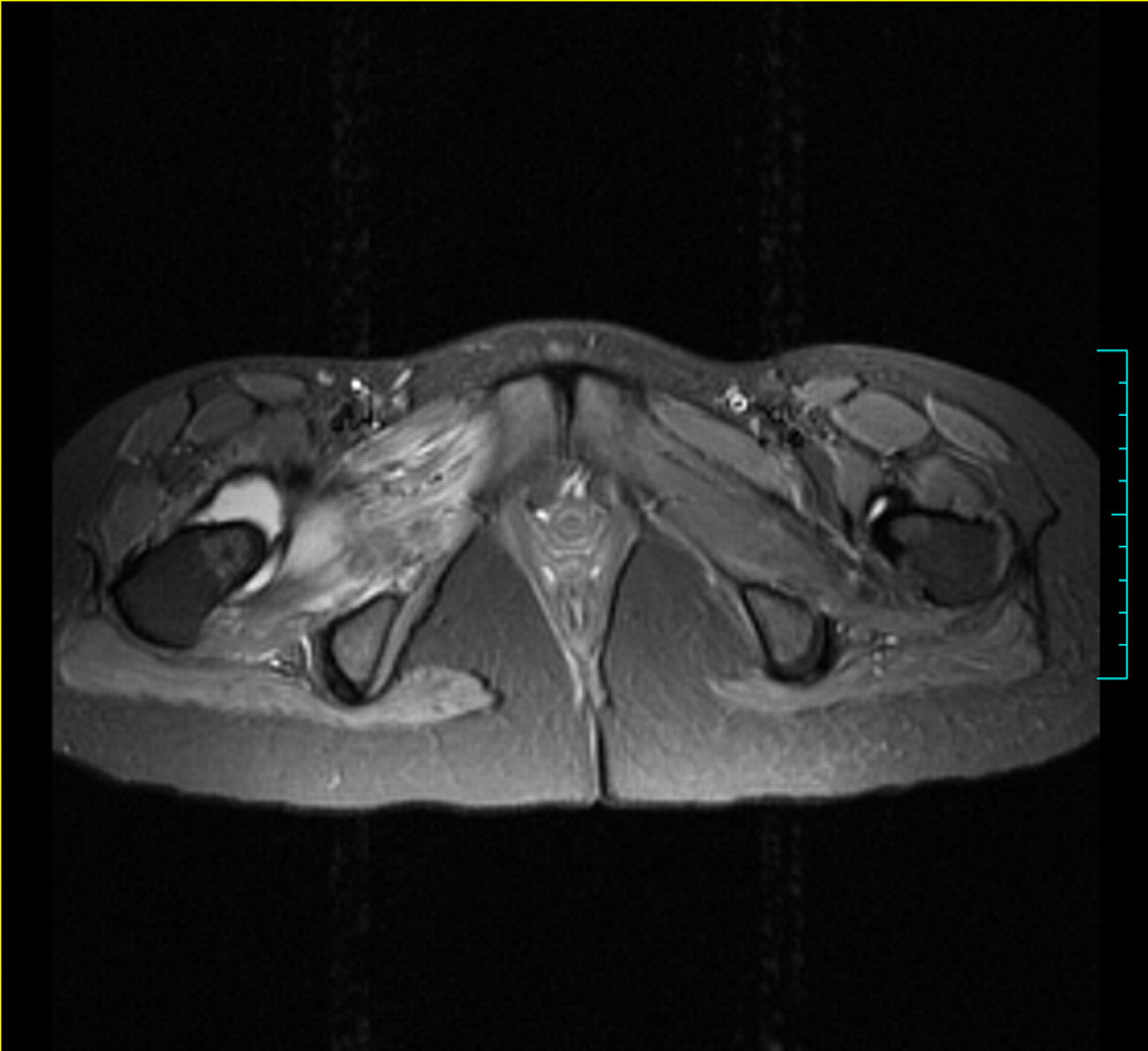
Early osteonecrosis of the right femoral head with effusion seen in an anterio-superior aspect of the right femoral head
Case 2
A 35-year-old woman had been diagnosed with SLE eight years earlier and subsequently underwent six cycles of cyclophosphamide chemotherapy and bilateral total hip replacement (THR) one year earlier. She was admitted with anterior dislocation of the right hip along with a fever of five days duration (Figure 2). The CRP level was 193mg/L on admission. The provisional diagnosis was infected right THR (septic arthritis) for which debridement was carried out. About 30 mL of pus was drained from under the tensor fascia lata in the joint and sent for culture and sensitivity testing. Her blood cultures were sterile throughout. She was started on cefuroxime and amikacin pending the culture reports. S. typhimurium, which was sensitive to all routine antibiotics, was isolated from the culture. Subsequently, she was started on ciprofloxacin and ceftriaxone. She was discharged after two weeks with advice to continue oral ciprofloxacin for the next four weeks. She is on regular follow-up and was last seen in September 2010 with no evidence of relapse.

Septic arthritis with anterior dislocation of right prosthetic hip
Discussion
Septic arthritis is a medical emergency and can cause rapid joint destruction resulting in permanent loss of joint function. Therefore, a delay in diagnosis and treatment may severely impact prognosis. Infectious aetiology must always be considered in a SLE patient, even when a diagnosis of chronic arthritis has been made. Salmonella septic arthritis is more commonly seen in young SLE patients with oligo-articular involvement and almost always involves the hip joint. 5 Both our patients were young women on steroids but with mono-articular involvement of the hip joint. The first patient had received steroids for only one month, while the second had received both steroids and six cycles of cytotoxic chemotherapy for over two years. Six weeks of therapy with cotrimoxazole, ampicillin, ceftriaxone, quinolones or chloramphenicol is recommended for salmonella bone infections. Quinolone therapy is preferred, especially for prosthetic joint infections. 6 Recovery of articular function in prosthetic joints is said to be superior in S. typhimurium septic arthritis compared to other Gram-negative counterparts. 7 Several studies have suggested the occurrence of elevated virulence and invasiveness of S. enterica and subspecies enterica Serovar Enteritidis and Typhimurium isolates. 1 Clinically, it is very difficult to differentiate between septic arthritis in its early stage from arthritis associated with underlying SLE delaying diagnosis. CRP levels in SLE patients are raised during exacerbations but studies have shown that a level greater than 50mg/L strongly suggests infection. 8 Both our patients had CRP levels greater than 50mg/L on admission. In a study on bacteraemia in SLE patients, salmonellosis was found in 40% while in non-SLE patients it was only 2%. 5 A recent study comparing salmonella and non-salmonella septic arthritis in SLE patients reported that 59% of all isolates belonged to Salmonella spp. with all of them being S. enteritidis B. S. aureus was the second most common isolate with 24% prevalence. The same study also reported that all the cases of salmonella septic arthritis also had concurrent bacteraemia with the same pathogen. 5 Only one of our patients had bacteraemia due to the same Salmonella spp. The interval from the diagnosis of SLE to the diagnosis of septic arthritis was 21 days in the first case and 96 months in the second case which is similar to findings reported in other case series (2–204 months). 5
Conclusions
Contrary to the popular belief that septic arthritis in SLE patients is polyarticular, our report highlights the fact that it should be considered even in patients who present with acute mono-articular joint involvement, particularly if the CRP levels are greater than 50mg/L. Empirical antibiotics with adequate coverage for salmonella and S. aureus, which are the most common organisms causing septic arthritis, should be considered and may later be modified based on the sensitivity of the cultured isolate. Hence, an early diagnosis and administration of the appropriate antibiotics is the cornerstone to the prevention of complications such as septicaemia and the permanent loss of joint function.