
Abstract
Road traffic injuries (RTI) are a rapidly growing public health problem in developing countries. This study was aimed at assessing the early outcome of RTIs received in our hospital emergency room. Understanding this will help to achieve optimum injury outcome. A prospective study was conducted on all patients presenting with RTIs to the emergency room of the Ebonyi University Teaching Hospital, Abakaliki, from 1 March 2007 to 29 February 2008. Out of 363 patients: 72.45% were treated in the emergency unit and discharged; 12.7% left against medical advice; 10.9% were admitted to the ward; and 4.7% died. Self-discharge against medical advice was significantly related to the type of injury (78.3% had fracture/dislocation) and gender (P = 0.001). The patronage of traditional bone setters, because of cultural belief that they have supernatural ability to treat fractures, was the major reason given by those who left against medical advice. The morbidity and mortality rate was significantly related to the road type (P = 0.005 – a higher rate was observed for RTIs received on intercity roads than intracity ones) and the type of crash (P = 0.03 – more than half from head on collisions). Although the mortality rate was within the expected range, the preventable death rate was high, and the majority of deaths occurred within the ‘golden hour’ . Improvement in pre-hospital and emergency room care of patients with RTIs, as well as public awareness of the availability and efficacy of orthodox orthopaedic trauma care, are needed in the developing countries.
Introduction
The adverse health outcomes of road traffic injuries (RTIs) are a heavy burden that can slow down the pace of growth and development in any nation that does not have appropriate policy responses to reduce road traffic accidents.
RTIs are ranked ninth in the global disease burden and are projected to be the third by 2020. 1 Low- and middle-income nations account for 85% of deaths due to RTIs. 1 Despite the under reporting of RTIs in Nigeria, the Federal Road Safety Commission's accident data show a fatality rate of 28 persons per 100,000 population; in 2008 alone, 6661 died and 27,980 were injured in RTIs. 2 Poor enforcement of road traffic safety regulation, the inadequacy of the public health infrastructures, poor access to health services and the increasing use of motor vehicles are factors that contribute to the high burden of RTIs in developing nations. 3
A lack of appropriate pre-hospital and hospital emergency room care are amongst the risk factors that influence post-crash outcomes. 4 In low income countries, only a small proportion of patients get pre-hospital care, and this is given mostly by bystanders and rarely by police or medically trained personnel. 5 A lack of appropriate infrastructure and equipment in hospitals can be a challenge when managing those patients who reach hospital alive. Mortality and recovery, with or without morbidity, are often the outcome for RTIs and an understanding of these outcomes is necessary in order to achieving the optimum care of injured patients.
Although there have been a lot of published reports on RTIs, only a few have focused on the outcome. 6–8 The aim of this study was to assess the early outcome of RTIs received in the emergency room of a teaching hospital in a developing country.
Patients and methods
This is a prospective study of the outcome of patients with RTIs who received treatment in the emergency room of the accident and emergency department of the Ebonyi State University Teaching Hospital (EBSUTH), Abakaliki, Nigeria, from the 1 March 2007 to 29 February 2008. EBSUTH is one of the major university teaching hospitals in Southeast Nigeria and is situated along a major interstate highway. It has the capacity to provide services to trauma patients and serves a population of about 8 million.
A questionnaire was designed with information relating to: the type of host (road user); the type of road (intra- or intercity road) on which the accidents occurred; the type of crash and the mechanism of the injury; the injury sustained; pre-hospital care; the duration between injury and presentation in the emergency room; the trauma score parameters; and the outcome of the injury. The injury severity score (ISS) and the trauma and injury severity score (TRISS) for each patient was computed using the trauma score parameters. The patients were categorized according to their placement (after resuscitation and treatment in the emergency setting) into one of the following outcome scales: died; admitted into the ward as an inpatient; discharged from the emergency room to the outpatient clinic; and self-discharged against medical advice (DAMA). The duration of the time between injury and death and the duration of admission by the time of death were also documented. The patients were followed up for mortality within 30 days of injury. The DAMAs were fully informed about the nature of their injuries and the definitive treatment they were to expect. Their reasons for DAMA were also documented.
With the approval of Ethics and Research Committee of the institution, data was collected by casualty officers and surgical residents.
Data was analysed using SPPS 10.0 statistical software for frequency tables and cross tables (SPSS Inc, Chicago, IL, USA). Chi square was used for the statistical test of significance and the P value <0.05 was considered significant.
Results
During the study period, 363 RTI patients were received in the emergency room (Figure 1). Of these, 263 (72.5%) were treated and discharged to the out-patient clinic, 46 (12.7%) discharged themselves against medical advice, 37 (10.2%) were admitted to the ward and 17 (4.7%) died.
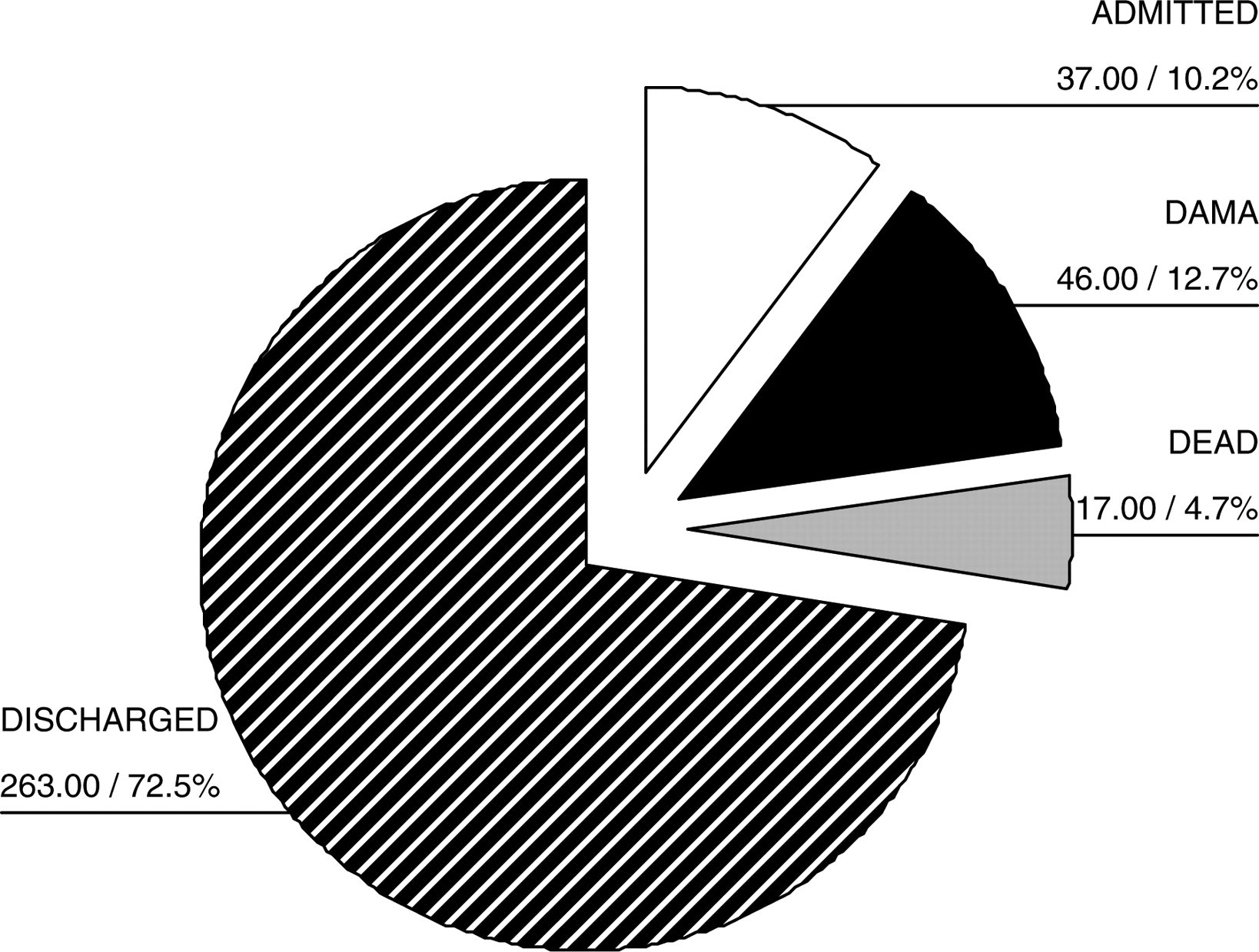
Outcome of road traffic injuries
The median duration of time between injury and arrival at the emergency room was 3 h. Extrication and transportation of patients to the emergency room were the aspect of pre-hospital care given to about 80% (290) of the patients by bystanders, police and members of the Federal Road Safety Corps. About 10% (36) were taken to the nearest community health centres for first-aid treatment before being transported to the hospital emergency room. None received medical care at the scene of the crash or en-route to the hospital.
Discharged to the out-patient clinic
The ISS in this group of patients ranged from 1–10; the median and the mean were 1 and 2.6, respectively. The 18–39 year group accounted for 66% of patients in this category (Table 1), and motor vehicle passengers accounted for a majority (35.0%) of them (Table 1). A significant proportion (P < 0.001) of patients discharged only sustained soft tissue injuries (Table 2).
Outcome by epidemiological factors
*Pearson χ2 [9 degree of freedom (df)] is 5.036 (P = 0.831)
†χ2 (15 df) 46.3 (P = 0.001)
‡χ2 (3 df) is 12.69 (P = 0.005)
DAMA, discharge against medical advice; MC, motorcycle; MV, motor vehicle
Outcome by type of crash and injury/severity
*
†Pearson χ2 [18 degree of freedom (df)] is 30.893 (P 0.03)
‡Pearson χ2 (18 df) P 0.001
§Includes multiply injured patients
DAMA, discharge against medical advice; MC, motorcycle; MV, motor vehicle
Self-discharged against medical advice
The ISS of this category of patients ranged from 2–25. The mean ISS was 12.7 and the median ISS was 13 (Table 2). Fourteen (30%) had ISS ≥16. There was proportionately more DAMAs amongst the men than the women (P < 0.01) Motorcycle drivers accounted for the highest proportion (38.9%) of the DAMAs (Table 1). There was a statistical significant difference between the type of injury sustained and the incidence of self-discharge (P < 0.001). Patients with fractures and/or dislocations, either in isolation or in association with another injury, accounted for 78.3% of the DAMAs (Table 2). Ten (21.7%) of these sustained open fractures of the extremities, 4 had type 3B, 5 type 3A and 1 type 11 Gustillo open fractures.
All patients in this group admitted that they were leaving the hospital to seek the services of traditional bone setters. The reason for this given by 37 patients (about 80%) was a strong cultural belief that fractures are better treated by traditional bone setters; 7 (15%) patients were afraid of the possibility of amputation in hospital; and the remaining 5% did not disclose their reasons.
Admitted into the ward
The ISS of patients admitted to the ward ranged from 8–34 with a mean of 15.7 and a median of 16 (Table 2). The probability of survival (TRISS) was ≥95% in 90%. The majority of those admitted (67.6%) were in the younger age group (Table 1). Admission was significantly related to the type of road – inter- and intracity roads accounted for 75.68% and 24.32% of the admissions, respectively (P = 0.005; Table 1). A majority of those admissions admitted to the ward (51.4%) had injuries caused by a head-on collision (Table 2). Motorcycle drivers accounted for 38.9% of the admissions while their passengers accounted for 13.9% (Table 2).
There was a significant difference in the number of patients admitted by type of injury (P < 0.001): fracture only, soft tissue only, soft tissue injury and fracture accounted for 30.6%, 27.8% and 25% of the admissions, respectively (Table 2). Patients with multiple injuries accounted for 48.64% of the admissions.
Death
The ISS of the patients who died was ranged from 16–75, the mean was 37 and the median was 29.5 (Table 2). About 82% (14/17) of those who died presented in the emergency room within the first 6 h of injury. About 60% of mortality occurred within the first 6 h of injury whereas about 10% within 6–24 h and about 30% after 24 h – 6 days. The duration of admission by the time of death was <1 h in about 47% (8/17), 1–6 h in about 12% (2/17), 7–24 h in 6%(1/17) and >24 h–6 days in about 35% (6/17). Eleven (65%) of these had a probability of survival (TRISS) ≥ 50%. Mortality was significantly related to the type of road (P < 0.005). About 59% of the deaths were due to road traffic crashes on intercity roads (Table1). There was a significant difference in mortality amongst road user types (P < 0.001; Table 1). Motorcycle drivers and motor vehicle drivers accounted for 35.3% and 11.8%, respectively. Motorcycle passengers, motor vehicle passengers and pedestrians accounted for 5.9%, 29.4% 11.8%, respectively, of the deaths. About 58.8% of those who died were in head-on collisions, whereas 11.8% of those who died were pedestrians (Table 1). There were significantly more mortalities among patients with both soft tissue injuries and fractures (71% of whom were multiply injured), and they accounted for 64.7% of deaths (P < 0.001). Patients with soft tissue injuries (31% of whom had multiple injuries) accounted for 29.4% of the mortality rate (Table 2).
Thirteen of the patients (76.5%) who died had head injuries either in isolation (8/13) or as part of multiple injuries (5/13). Motorcycle drivers and their passengers accounted for 61.5% of those who died from a head injury. Two patients died as a result of a chest injury (tension pneumothorax), and the remaining two died from hypovolaemic shock resulting from a severe haemorrhage.
Discussion
In developing countries, tertiary injury prevention mechanisms aimed at optimizing the outcome of injuries has been seriously set back due to inadequate health infrastructures. The result of our study indicates that 263 patients (72.4%) were treated in the emergency unit and discharged to the out-patient clinic. This is a little more than the 61% reported by Alissa in Amman, Jordan. 9 The emergency and outpatient care given to this volume of patients in a year places a heavy burden on the already stressed health infrastructures. A majority of the patients (90.1%) who were discharged sustained only soft tissue injuries – mainly lacerations, abrasions and contusions that could be sorted out in the emergency unit and followed up in the outpatient clinic.
DAMA is not uncommon amongst traumatized patients in our environment. The proportion of RTI patients who left against medical advice in our study was 12.7%. This was lower than the 29.8% reported by Solagberu et al. in a teaching hospital in North Central Nigeria. 10 Solagberu's study was on motorcycle injuries and, interestingly, motorcycle riders were the highest proportion (39.1%) of road users who DAMA in our study (Table 2). The result of this study also showed the highest proportion of DAMAs were patients with fractures/and dislocation (P < 0.001; 78.3%; Table 2). All of the DAMAs admitted that they wanted to seek the services of traditional bone setters. The patronage of traditional bone setters (indigenous people without formal medical training but who are easily accessible to patients with extremity injuries) and other unorthodox healers reported in other studies has been the major reason for DAMA. 10 A majority of patients in our study who left for the services of traditional bone setters did so because of a strong cultural belief that traditional bone setters have a supernatural ability to treat fractures.
That 30% of the DAMAs were severely injured (ISS ≥ 16) and that 10 (21.7%) had severe open fractures suggests a gross underestimation of injuries and a high level of ignorance about the availability and efficacy of orthopaedic trauma care amongst this category of patients. This is a serious public health problem that calls for aggressive public enlightenment about the efficacy and availability of orthodox orthopaedic trauma care. Health-care service interventions in RTIs are aimed at achieving the optimum injury outcome (tertiary prevention). Achieving an optimum outcome after injury is unlikely in a setting in which the injured, out of ignorance, do not accept orthodox treatment. The complications arising from poorly managed injuries of the extremities (gangrene, non-union of fractures, chronic post-traumatic ulcers, etc.) by traditional bone setters and unorthodox healers, which other studies have documented, 11–14 might be an important and under-recognized factor in the adverse health outcome of RTIs in the sub-region.
Admission to the surgical ward from the emergency room is a reflection of the seriousness of an injury as observed from the median ISS of 16. Our study indicates that 10.19% of patients were admitted to the ward, which is in contrast to 37% of about the same number of patients reported by another study. 9 The lower percentage of admissions in our study may be due to the proportion that merited admission but discharged themselves against medical advice. The result of our study indicates that the number of admissions was significantly related to intercity roads, and this was similar to the increased severity of injury on the same type of roads recorded by Afukaar et al. in Ghana. 13 Another study is needed in order to determine the reasons for the higher rate of morbidity observed on our intercity roads.
The mortality of 4.7% in our study is the proportion of patients with RTIs who died after they were received in the emergency unit. This figure did not include those who died at the scene of crash, at home or under the care of unorthodox healers. The mortality rate of 4.7% is within the expected worldwide range (0.5–6%) and more or less similar to those recorded by other studies. 9,14 The result of our study also indicates that young people accounted for 70.6% of the mortality rate, higher than the 50% reported by Dandona and co-workers in India. 15 In addition, the younger age group accounted for the majority of admissions in our study. This implies a loss in productivity which perpetuates the existing cycle of poverty and disease in the developing nations.
It was observed that mortality was proportionately greater amongst motorcycle drivers and passengers than other road users in our study. It was also observed that most of the injuries from head-on collision, pedestrians and side collisions involved motorcycles. A majority of head injury-related deaths occurred among motorcycle drivers and their passengers, which could be explained by a lack of crash-helmet use by motorcyclist and the non-enforcement of the crash-helmet law in Nigeria (at the time of this study). This has been documented in another study. 10 In Nigeria, the virtually non-availability of driving schools for prospective motorcycle drivers compared to four-wheel motorized vehicle drivers compounds the situation.
Most deaths occurred within the ‘golden hour’, i.e. the second peak of the Trunkey trimodal pattern of mortality following severe trauma. Death within this period is preventable where there is an accessible and competent accident and emergency system. 16 The results of our study also indicate that 11 (65%) of those who died had a greater than 50% probability of survival, which implies a preventable death rate of 65%. The high probability of survival of these patients despite their severe injuries (ISS >16) is a reflection of the inadequacies of the emergency health-care services in Nigeria, which other previous studies have also documented. 10 There is also an insufficient number medically trained personnel who can give treatment at the scene of a crash, en-route to the hospital and in the hospital emergency room. Medical care such as simple first-aid measures at the scene of crash and en-route to hospital could have prevented deaths from haemorrhagic shock, tension pneumothorax and airway obstruction in unconscious head injured patients.
The limitations of this study are:
It was a single centre study, and data obtained may not be representative of the entire population; It is a hospital-based study, and some of the casualties of road traffic crashes who sustained minor injuries may not have presented to the emergency room; We were unable to obtain reliable information on alcohol consumption.
Conclusion
The mortality rate of RTIs received in our emergency unit was within the expected range, although the preventable death rate was high. DAMA was significantly related to the fracture/dislocation type of injury. A strong cultural belief that traditional bonesetters have a supernatural ability to treat fractures was observed in a majority of DAMAs. The care of patients injured in road traffic accidents can be improved by prompt resuscitation in the emergency room, as well as by proper medical care at the scene of the road traffic accident and en-route to the hospital in developing countries. A programme should be instituted in developing countries that will provide the public with information about the availability and efficacy of orthodox orthopaedic trauma care.
Footnotes
Acknowledgment
We thank all who assisted in this study.