
Abstract
We undertook this study in order to determine the current role of digital rectal examination (DRE) in the diagnosis of prostate cancer in a resource-poor setting. The diagnosis of prostate cancer has been revolutionized by the introduction of prostate-specific antigen (PSA), transrectal ultrasound (TRUS) for biopsy guidance and more efficient biopsy equipment, but they are not readily available in most developing countries. This is a prospective study of 131 patients with suspected prostate cancer based on clinical presentation, DRE and elevated PSA. The presence or absence of cancer was confirmed by biopsy and histologic examination. Patients with screen- or incidentally-detected prostate cancer were excluded. The most common symptom was the development of lower urinary tract symptoms (LUTS). All patients had abnormal DRE and indurated prostate was the most frequent finding (50%). The mean PSA was 33.9ng/mL: of the 131 patients, 80 (61.1%) had a malignant histology following biopsy, 47 (35.9%) were benign and four (3.0%) were prostate intraepithelial neoplasia (PIN). The low specificity of DRE in the diagnosis of prostate cancer requires that it should be combined with other diagnostic modalities such as PSA and TRUS-guided prostate biopsy. Thus government and health-care providers in resource-poor countries must strive to make these facilities available in order to improve prostate cancer diagnosis.
Introduction
Worldwide, prostate cancer is the fourth most commonly diagnosed malignancy affecting men beyond middle age. The age adjusted incidence is 149/100,000 person years in African-Americans, 108/100,000 in Caucasians, 1 127/100,000 in Nigerians, 2–4 and 28/100,000 in Orientals. 1 The diagnosis of carcinoma of the prostate has been revolutionized by the introduction of prostate-specific antigen (PSA), transrectal ultrasound scan (TRUS) and the availability of efficient biopsy equipment.
Prostate cancer rarely causes symptoms until it is at an advanced stage and, thus, a suspicion of cancer that results in the recommendation for biopsy is most often raised by the findings of elevated serum PSA and/or an abnormal digital rectal examination (DRE). 5,6 At the time of diagnosis only 55% of tumours are clinically localized where there is no organized screening but with screening more than 95% are diagnosed in the early stages of the disease. 7,8 In the developing communities, the majority of patients present late with either locally advanced or metastatic disease. 2,4 Although the specificity of DRE is low it increases with the stage of prostate cancer. Thus patients with significantly elevated PSA and abnormal DRE findings are more likely to have reached a higher stage of disease with increased morbidity and mortality. This implies that where prostate cancer diagnosis relies mainly on clinical suspicion and abnormal DRE, early prostate cancers are likely to be missed. Health-care institutions in most sub-Saharan African countries, and some other developing countries, lack these advanced diagnostic facilities and, therefore, rely on clinical suspicion and DRE for the diagnosis of prostate cancer.
Methods
This is a prospective study that was carried out over a period of 15 months (September 2007 and December 2008) at Ahmadu Bello University Teaching Hospital, Zaria. Approval for the study was obtained from the Hospital Ethical and Scientific Committee before the commencement of the study. Only patients who willingly consented after counselling were included in the study. The study is based on a routine investigative procedure for all patients with suspected carcinoma of the prostate. Any additional cost incurred outside the routine treatment for this study was borne by the investigator.
The patients used in this study were those who presented to either the outpatient clinic or the accident and emergency unit and who required a prostate biopsy in order to confirm the presence of cancer. The inclusion criteria were: clinical presentation suspicious of prostate cancer; abnormal DRE and TRUS findings with elevated PSA. The suspicion of cancer on DRE included the feeling of areas of indurations, hard or craggy feel, asymmetry and presence of nodules. Patients who were severely ill and debilitated who could not withstand biopsy, patients with suspected early disease and those who had had any form of treatment for prostate cancer were excluded from the study. Data obtained was analyzed using SPSS (Statistical Package for Social Sciences) computer software. The results were displayed in tables and charts.
Results
A total of 131 patients met the inclusion criteria and were enrolled into the study. The mean age was 66.3 years with a range of 49–91. The age interval 60–69 years accounted for most of the patients (59, 45%). The age distribution is shown in Figure 1.

Age range distribution of the patients
The most common reason for presentation was due to lower urinary tract symptoms (LUTS) in 87 (66.4%). Other symptoms are shown in Table 1.
Distribution of symptoms at presentation
LUTS, lower urinary tract symptoms
The patients all had either one or more physical examination findings of advanced disease (locally or metastatic) as shown in Table 2.
Other clinical examination findings
The findings on digital rectal examination which indicated a suspicion of prostate cancer showed: an indurated prostate in most of the patients, 65 (50%); hard/craggy prostate in 36 (27%); and 30 (23%) had nodular prostate (see Figure 2). The mean PSA was 33.9 ng/mL (range 10.2–120) with a standard deviation (SD) of 19.33.
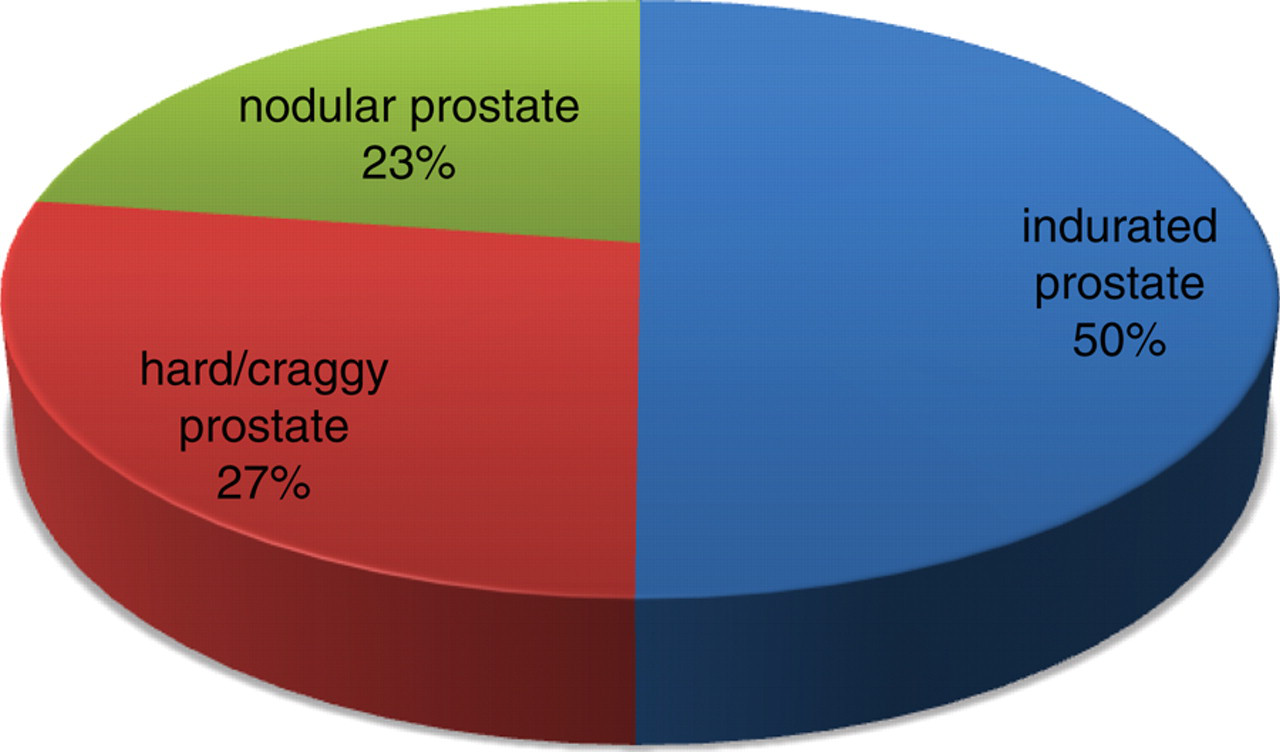
Findings on digital rectal examination
Of the 131 patients: 80 had malignant histology following biopsy; 47 were benign; and prostate intraepithelial neoplasia (PIN) was found in four. Thus the specificity of DRE for detecting cancer was 61.1%, as shown in Table 3.
Digital rectal examination and histologic outcome
PIN, prostate intraepithelial neoplasia
Discussion
The diagnosis of prostate cancer has witnessed remarkable improvements in the last two decades – the introduction of PSA and the development of efficient biopsy equipment guided by TRUS have had the most impact. These advancements led to an increase in the incidence of prostate cancer. 6,7 However, there was a concomitant decrease in cancer-specific morbidity and mortality because early and potentially curable stages of disease became the most common. 7 In contrast, in most developing communities where these facilities are yet to be readily available, the majority of patients with prostate cancer are diagnosed at an advanced stage with an attendant higher morbidity and mortality. 2 In these communities, DRE continues to play a major role in prostate cancer diagnosis as the initial clinical evaluation and digital guidance of prostate biopsy. In this study, the majority of patients fell within the 60–69 age range which is consistent with findings by Osegbe 2 and other Nigerian works. 3,4
The suspicion of prostate cancer necessitating confirmation by biopsy commonly follows the development of symptoms of local or advanced disease with abnormal DRE findings. Suspicious DRE findings include: a nodule; asymmetry; difference in texture (firm, hard or craggy); and fixity to rectal mucosa. 5 False-positive DRE can be a result of the following: a change in consistency as a result of prostatitis; benign prostatic enlargement; calculi; TB; schistosomiasis; and prostatic infarct. In this study most of the patients had symptoms and signs which led to a suspicion of either local or advanced disease with abnormal DRE. However, only 80 of the 131 patients were found to have prostate cancer after biopsy (Table 3). Though a repeat (especially extended or saturated TRUS-guided biopsy) may reveal more cancer among the initially negative group, the low specificity of DRE is evident. Normal DRE is also found in many patients who harbour prostate cancer. Thus, a reliance on DRE as a sole trigger for prostate biopsy will lead to under-diagnosis.
The specificity of diagnosis of carcinoma of the prostate on DRE is 30–50%. 8,9 The low positive predictive value for cancer of DRE alone requires the need for a combination with other screening modalities (serum PSA and prostatic biopsy) in order to be able to establish a diagnosis. 7,8 The risk of positive DRE turning out to be cancer is heavily dependent on the PSA-value. 10 The probability of detecting prostate cancer with increasing serum PSA has been reported by some studies: for a PSA level of 0–1 ng/mL, the positive predictive value (PPV) for cancer is 2.8–5%, for 1–2.5 ng/mL, the PPV is 10.5–14%, while for 4–10 and >10 ng/mL the PPV is 41 and 69%, respectively, showing a clear increasing cancer yield with rising PSA value. 10 It should also be noted that only about 33.3% of prostatic nodules palpable on DRE are positive for prostate cancer. 9 With increasing screening, and consequent cancer detection at an early stage, most patients diagnosed with carcinoma of the prostate have normal DRE results.
The patient selection criteria in this study excluded patients who might harbour prostate cancer but had normal DRE findings with only an elevated PSA. This group of patients accounted for screen- or incidentally-detected prostate cancers and they commonly have an early disease which is potentially curable with lower morbidity and mortality. The specificity of DRE in this study is 61.1%, which is higher than that reported by most investigators. However, this is attributable to our patient selection, i.e. patients that were symptomatic had abnormal DRE and markedly elevated PSA with most also having features of a locally advanced or metastatic disease. Any meaningful effort aimed at reducing the morbidity and mortality of prostate cancer should be focused on early detection. There are limitations to the use of DRE for prostate cancer diagnosis, they include low sensitivity and specificity and subjectivity with a high interexaminer variability. 9,11 As DRE is no longer used as a sole tool for prostate cancer screening or diagnosis, because of its low specificity, it must be combined with other modalities for diagnosis such as PSA, TRUS and biopsy. 12,13 The old digitally-guided biopsy has been replaced by TRUS-guided biopsy which is now the gold standard. 14 However, DRE is still useful in clinical staging of prostate cancer, monitoring of treatment and follow-up. There is a need for government and health-care providers in these communities to acquire the new facilities in order to improve prostate cancer diagnosis and treatment. However, the limitations of policies, funds and health-care priorities remain the major impediments.
Conclusion
The low specificity of DRE implies that it is unreliable as a sole tool of prostate cancer diagnosis and, therefore, it should be combined with other diagnostic modalities such as PSA and TRUS-guided prostate biopsy in order to improve the yield.
Government and health-care providers in resource-poor countries must strive to make these facilities available in order to improve prostate cancer diagnosis and, thus, reduce the morbidity and mortality associated with the disease.