
Abstract
Summary
Tuberculosis (TB) of the rib is a very rare form of skeletal TB and its diagnosis may be difficult because of a low index of suspicion by clinicians. The presentation often mimics malignant disease clinically and radiologically and diagnosis may only be confirmed by tissue biopsy. We present a 32-year-old HIV-negative man who presented with a three-month history of progressively worsening pleuritic chest pain, weight loss, fatigue, anorexia and low-grade fever with night sweats. A chest computerized tomography (CT) scan showed destructive lesions in the right fourth and seventh ribs with no pulmonary lesions. A diagnosis of TB of the rib was made after surgical resection and histopathology of the affected tissue. There was significant improvement when anti-TB therapy was initiated. This case report emphasizes the importance of a high index of suspicion of TB in patients presenting with destructive bone lesions in regions with high prevalence of TB.
Introduction
Tuberculosis (TB) of the rib is a rare form of skeletal TB occurring in only 0.1% of all TB infections. 1 Diagnosis is often difficult because of the low clinical suspicion and because presentation often mimics malignant disease 2 resulting in delayed or missed diagnosis with subsequent devastating deformities and functional deficits.
Case summary
A 32-year-old man was admitted with a three-month history of progressively worsening right pleuritic chest pain, weight loss, fatigue, anorexia and low-grade fever with night sweats. He had a dry cough two months prior to admission which subsided a week later after taking oral antibiotics. He reported no subsequent cough or haemoptysis. He denied any history of previous TB and the family history of TB was negative. He reported no chronic illness and no history of smoking, alcohol consumption or drug abuse.
On physical examination, he appeared wasted but was afebrile. Chest movement was minimal because of right chest pain. There was tenderness to palpation over the right axillary area but no swelling and auscultation revealed a pleural rub. The rest of the examination was unremarkable.
Investigations
Laboratory findings included a negative HIV antibody test, normal complete blood count and serum biochemistries and negative aerobic blood cultures. C-reactive protein (42.39 mg/L) and erythrocyte sedimentation rate (110 mm/h) were raised. The Ziehl-Neelsen (ZN) sputum smear was negative for acid-fast bacilli.
A chest radiograph showed a wedge-shaped opacity arising from the pleura in the right mid-lung zone. Chest ultrasound scan confirmed a cystic mass (4.3 cm by 2.7 cm) in the right pleural space with normal adjacent tissue. Aspiration of the cystic mass revealed purulent material. Microscopy using Gram's stain and ZN stain was negative and so was aerobic culture. Cytology of the aspirate was negative for malignancy. A chest computerized tomography (CT) (Figure 1) showed a fusiform-shaped mass (4.8 cm by 2.7 cm) in the right fourth intercostal space extending to the pleura with destructive lesions in the fourth and seventh ribs and no pulmonary lesions. Serum-protein electrophoresis and Bence-Jones proteins were negative. With a presumptive diagnosis of malignant osteolytic lesions complicated by a chest wall abscess, antibiotics were given and he underwent surgery for biopsy and drainage. Intraoperatively, a cystic mass (3 cm by 10 cm) in the right fourth intercostal space, extending to the pleura with destruction of the fourth rib and caseous necrosis in the underlying soft tissue was found. Resection of the rib and cystic mass was done and a chest drain was left in situ. Histopathology of the excised tissue showed granulomatous inflammation with a giant cell reaction and no malignancy (Figure 2).
A chest CT scan showing a fusiform-shaped mass in the right fourth intercostal space extending to the pleura (white arrow) with early destruction of the inferior aspect of the fourth rib (black arrow)
Microscopic examination of the tissue biopsy showing granulomatous lesions (A: i, ii and iii), giant cell (B, arrow) and bone necrosis (C)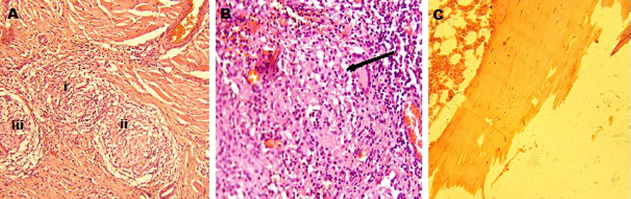
A diagnosis of TB of the rib cage involving the fourth and seventh ribs with a cold abscess was made. He recovered well after two months of isoniazid, rifampicin, ethambutol and pyrazinamide followed by six months of rifampicin and isoniazid.
Discussion
Skeletal TB is uncommon in immunocompetent individuals. 3 This report describes an unusual form of skeletal TB – TB of the rib – in an individual with no underlying immunosuppressive condition. Only a few cases of TB of the rib in immunocompetent individuals have been reported,4–5 the majority of which had a positive previous history of pulmonary TB (PTB) or active PTB at presentation: our patient had neither. TB is the second cause of rib destruction after metastases but is rarely suspected by clinicians. Our patient had destructive bone lesions which made the diagnosis elusive as such a presentation is more suggestive of malignant disease. The diagnosis was only confirmed after surgical resection and histopathology. Our experience is consistent with other published cases where the diagnosis was made after surgery. 2
Conclusion
We emphasize the importance of a high index of suspicion of TB in patients with destructive bone lesions in regions with high prevalence of TB.
Footnotes
The authors declare no conflict of interest.
Acknowledgments
The authors thank Professor Walter Schlech who edited this case report, Dr Sam Kalungi who assisted with the images, the patient who permitted us to write up the report and, lastly, the Infectious Diseases Institute, Makerere University for their scientific support.