
Abstract
Summary
Fifty children (mean age 8 years) with an absolute eosinophil count ranging from 1956 to 28,500 were studied in a tertiary hospital in Nepal. Most had multisystem involvement: 47 had constitutional symptoms; 38 had gastrointestinal symptoms; and 37 had respiratory symptoms. Abdominal pain, fever, cough and weight loss were the most common presentations while pleural effusion, ascites, pericardial effusion, abdominal nodes and high erythrocyte sedimentation rates were the common investigational findings.
Introduction
An abnormal accumulation of eosinophils in the blood or tissue can have profound clinical effects. The most important cause of eosinophilia worldwide is parasitic disease, while in industrialized nations it is atopic diseases. 1 Moderate-to-severe eosinophilia occurs as a response to helminthic parasitic infestation. 2 Among the parasitic infestations causing marked eosinophilia are Toxocara; filariasis leading to tropical pulmonary eosinophilia, Paragonimus westernmani, Gnathistoma spinigerum and Fasciola hepatica.
As the diagnostic tests for definite diagnosis of any of these conditions are not available in Nepal, it is important to diagnose the condition clinically. There has been no published data on the subject in our paediatric population. The disease burden is unknown and children have been the silent sufferers. We, therefore, planned a small study with the objective of discovering the diversity of symptoms and signs in children with moderate-to-severe eosinophilia secondary to parasitic infestations.
Materials and Methods
A prospective hospital-based descriptive study was carried out over a two-year period (5 April 2009 to 14 April 2011) at Patan Hospital, Patan Academy of Health Sciences, Patan, Nepal. Children with an absolute eosinophil count (AEC) of more than 1500/mm3 coming to the paediatric referral clinic or admitted to the paediatric ward were included in the study. Those with mild eosinophilia and those with other clinical conditions known to cause moderate-to-severe eosinophilia were excluded.
Informed verbal consent was taken from the children and their parents. The antiparasitic treatment chosen was based on clinical suspicion and children were followed up for 9–11 months.
Data was analysed using SPSS system (SPSS Inc., Chicago, IL, USA). Ethical approval was taken from the Institutional Review Board, Patan Academy of Health Sciences (IRB, PAHS) (Ref 2011.108.js).
Results
A total of 50 children, 39 boys and 11 girls, who fulfilled the inclusion criteria were enrolled. Their mean age was eight years. Seventy-two percent of them belonged to Tamang and Lama castes. Eighty-two percent gave a history of eating undercooked fresh water crab.
Fourteen children had moderate eosinophilia (AEC of 1500–5000/mm3) and 36 had severe eosinophilia (AEC of >5000/mm3). Their AECs ranged from 1956 to 28,500 (median, 9020; interquartile range [IQR], 8730). Forty-seven children had constitutional symptoms; 38 had gastrointestinal symptoms; 37 had respiratory symptoms; and 11 had cardiovascular symptoms. Abdominal pain (34), fever (32), cough (30) and weight loss (28) were the most common presentations (Table 1). Almost all had more than one symptom and more than one system was involved. The duration of the symptoms ranged from less than seven days to more than six months.
List of symptoms among the study children

Subcutaneous nodules were seen in four children and limb swelling with non-pitting oedema in another four children.
Eighteen children were moderately underweight and nine were severely underweight; 16 had moderate and 17 had severe stunting. There was no correlation between the weight and height Z scores and the AEC values.
Half of the children had an erythrocyte sedimentation rate (ESR) of more than 50 mm/h. The correlation between high ESR and AEC was significant (P = 0.015). All the children took a Mantox test and there were two positive results. Pleural and pericardial effusions were seen in 33 and 11 children, respectively; ascites (clinical and ultrasonological) was noted in 20; abdominal ultrasound revealed enlarged abdominal nodes in 11; 10 had an enlarged liver; two had a liver abscess; bone marrow aspiration was performed in six; and all showed increased eosinophilic precursors.
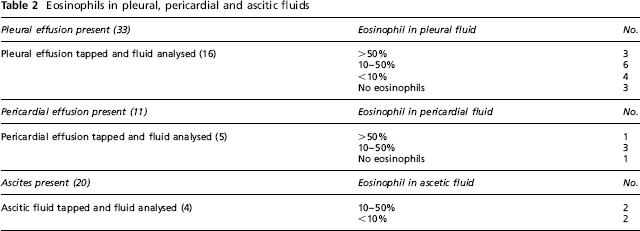
Sixteen of the 33 children with pleural effusion, five of the 11 with pericardial effusion and four of the 20 with ascites underwent pleural, pericardial and ascitic fluids aspiration and analysis. Eosinophilia was observed in 13 of 16 pleural fluids, four out of five pericardial fluids and all four of the ascitic fluid analysed (Table 2).
Eosinophils in pleural, pericardial and ascitic fluids
Following antiparasitic treatment (praziquantal, albendazole, diethylcarbamazine – either alone or in combination), most children showed symptomatic improvement (complete in 35 and partial in 8) and a gradual decline in AEC was observed (complete resolution of eosinophilia in 9 and a significant fall in AEC in 11).
Discussion
Moderate-to-severe eosinophilia secondary to parasitic infestations in children can present with non-specific symptoms involving different organ systems. As the diagnoses in many of these children have been delayed for weeks to months, they are made to suffer for prolonged periods and, hence, most were found to be underweight and stunted. In our study the predilection of moderate-to-severe eosinophilia in a particular ethnic group/caste (Tamang and Lama) could be due to their food habits (i.e. eating crab meat, which is common among this ethnic population).
Paragonimiasis is common in Southeast Asia, South America and Africa with 21 million people infected worldwide. 3 Human infection by P. westermani is endemic in East Asian and Southeast Asian countries.4,5 It is acquired by the consumption of raw or partially cooked crayfish and crabs. 6 In our study 82% of the children had a history of eating undercooked fresh water crab.
Human toxocariasis is ranked among the most common zoonotic infections worldwide and is common in toddlers with pica or exposure to puppies. 7 Hepatosplenomegaly plus evidence of multisystem disease and a history of pica make the diagnosis of toxocariasis (visceral larva migrans) very likely. 8 Almost a quarter of the study population were younger than five years old and many of them had multisystem involvement. In Nepal it is common to see toddlers playing on the ground and exposure to puppies is very common. Although we do not have data on tropical pulmonary eosinophilia in Nepali children, the population prevalence of lymphatic filariasis is high and is more common in certain districts of Nepal.9,10 Given the epidemiological risk for these parasitic infestations, suggestive clinical pictures and the clinical response to antiparasitic treatment there is a high likelihood that these infestation are the cause of hypereosinophilia in Nepali children.
Conclusion
The clinical presentation of children with marked eosinophilia secondary to parasitic infestations is non-specific. Diagnostic tests are not always easily available and, in the absence of diagnostic tests, a diagnosis can be made based on a high index of suspicion. A larger study that looks at the disease burden that attempts to identify the definitive parasitic causes is urgently needed.
Footnotes
None.