
Abstract
Summary
The objective of this study was to study the spectrum of neurological manifestations in patients with dengue infection. This was a prospective study undertaken at the Departments of Medicine and Neurology, Christian Medical College, Ludhiana, India. All patients diagnosed with dengue fever during an epidemic (1 September 2010–31 December 2010) were screened for neurological manifestations. There were a total of 799 patients with dengue infection. Neurological manifestations were present in 21 (2.63%),19 of whom were men with a mean age of 33.7 ± 13.9 years. The neurological diagnoses were hypokalaemia with: quadriparesis (7); myositis (4); encephalopathy (4); Guillain–Barre syndrome (2); acute disseminated encephalomyelitis (2); lumbosacral plexopathy (1); and intracranial haemorrhage (1). Three of these patients died. Clinicians should be aware that neurological manifestations in dengue fever are not uncommon.
Introduction
Dengue virus belongs to the family flaviviridae. It manifests as a spectrum of illness ranging from flu-like illness to devastating haemorrhages and shock (dengue shock syndrome). The pathogenesis involved are thrombopathy, vasculopathy and coagulopathy.
Various non-haemorrhagic cardiac and neurological manifestations have been noted. The neurological involvement in dengue virus infection is not uncommon. However, encephalitis, acute disseminated encephalomyelitis (ADEM), transverse myelitis, Guillain–Barre syndrome (GBS), myositis and stroke have been reported.1,2
There is paucity of data regarding the neurological manifestations in dengue patients from developing countries where there is the greatest prevalence of dengue virus infection. Hence, we conducted this prospective study.
Materials and Methods
This was a prospective study conducted at the Departments of Medicine and Neurology in the Christian Medical College, Ludhiana, a tertiary teaching institution in North West India. The study was carried out during an epidemic of dengue virus infection from 1 September 2010 to 31 December 2010. The diagnosis of dengue disease was based on: epidemiological (the post-monsoon period in an endemic area); clinical picture and laboratory investigations consistent with dengue infection (fever, body ache, thrombocytopenia; positive serum immunoglobulin M [IgM], enzyme-linked immunoadsorbent assay [ELISA]; or nonstructural protein 1 [NS1] antigen). 3 All patients were screened for neurological manifestations, received a clinical examination and had provided a detailed medical history.
The laboratory tests included: complete blood profile; serial platelet counts; transaminases; dengue NS1; and dengue IgM. Creatinine phosphokinase was tested in patients with severe muscle pains. Dengue IgM was detected using Pan Bio capture ELISA (< 9 Pan Bio units was negative; 9–11 was equivocal; and >11 was positive). The sensitivity of the test was 85.4–98.9% and the specificity was 95.7–100%.
Magnetic resonance imaging (MRI) brain, electromyogram (EEG) and nerve conduction studies (NCS) were carried out when indicated. The patients were managed as per the World Health Organization guideline. 3 Patients with haemorrhagic manifestations were given platelet rich concentrates as necessary.
Statistical analysis
Statistical analysis was done with SPSS version 16 (SPSS Inc., Chicago, IL, USA). The statistical measures used were frequencies and descriptive statistics. Quantitative variables were expressed as mean±standard deviation (SD).
Results
Neurological manifestations were noted in 21 (263%) of the 799 patients who were diagnosed with dengue virus infection. There were 19 men and the mean age was 33.77 ± 13.94 years.
All the patients had a history of fever with a mean duration of 4.52 ± 2.77 days. Bleeding manifestations were noted in five patients (1 gum bleeding; 2 haematuria; 1 haematochezia; 1 upper gastrointestinal bleed). The various neurological manifestations and investigations are shown in Table 1.
Clinical features and investigations
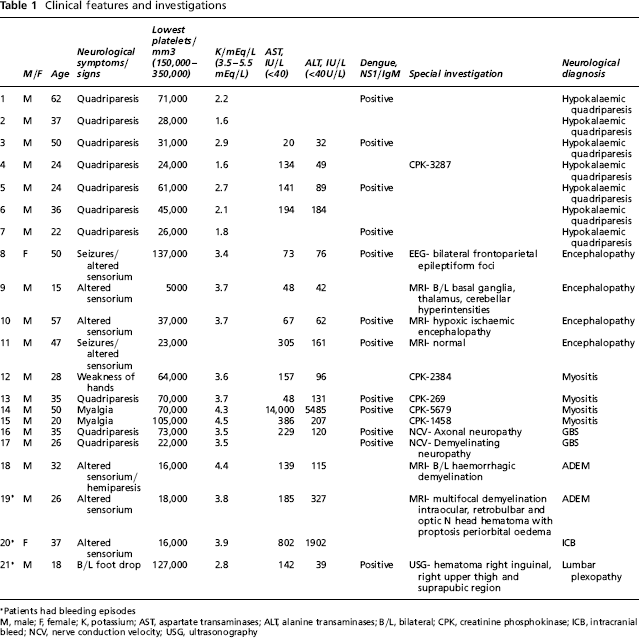
Patients had bleeding episodes
M, male; F, female; K, potassium; AST, aspartate transaminases; ALT, alanine transaminases; B/L, bilateral; CPK, creatinine phosphokinase; ICB, intracranial bleed; NCV, nerve conduction velocity; USG, ultrasonography
Hypokalaemic paralysis
Seven patients presented with acute pure motor flaccid quadriparesis (potassium levels ranged from 1.6 meq/L to 2.8 meq/L) with complete recovery of motor deficits after 12–48 h of potassium replacement.
Myositis
Myositis was diagnosed in four patients based on creatinine phosphokinase (CPK) values, of whom two had quadriparesis. The CPK values ranged from 269–5697 U/L (normal range, 24–195 U/L; Table 1). Electromyography (EMG) was not performed due to the low level of platelets.
Encephalopathy
Seizures were present in three of the four patients who had encephalopathy. EEG revealed disturbances in the frontal and fronto-parietal regions.
GBS
One of the two patients with GBS had bilateral VII nerve paralysis. Nerve conduction studies (NCS) showed demyelinating neuropathy in one and axonal neuropathy in the other.
ADEM
The two patients diagnosed with ADEM on MRI presented with hemiparesis with horizontal gaze palsy, quadriparesis with proptosis and VII nerve palsy. The MRI revealed bilateral haemorrhagic demyelination in one and demyelination along with intraocular, retrobulbar and optic nerve head haematoma in the other.
Lumbar plexopathy
One patient had bilateral foot drop secondary to lumbar plexopathy. His ultrasound revealed a haematoma in the right inguinal, the right upper thigh and the suprapubic region. Lumbar plexopathy was either secondary to a haematoma causing compression or may have been a result of the neurotropic effect of the virus itself.
Intracranial haemorrhage
Another patient presenting with upper gastrointestinal haemorrhage had a sudden loss of consciousness with unequal pupils, presumably due to intracranial haemorrhage (ICH) in the hospital to which she succumbed.
Laboratory findings
The mean haemoglobin levels at presentation were noted to be 13.09 ± 3.034 g/dL. The mean platelet count noted on the first day of presentation was 41,266.7/mm3 and in the next two days were 47,307.69/mm3 and 68,100/mm3, respectively. The lowest platelet count noted was 5000/mm3.
A total of 12 patients were laboratory confirmed cases of dengue (dengue NS 1/dengue IgM; Table1).
Outcome
Three of the 21 patients with neurological symptoms died. The neurological diagnoses for these patients were encephalopathy, ADEM and intracranial haemorrhage, respectively (cases 9, 18 and 20; Table 1). The patient with lumbosacral plexopathy had moderate disability at 1 month but, thereafter, made a complete recovery.
Discussion
Dengue infection is widespread in the tropics. The incidence of neurological manifestations in patients diagnosed with dengue haemorrhagic fever has been documented to vary from 3% in prospective dengue haemorrhagic fever studies to 25% in retrospective studies. 4 In our study the incidence was 2.63% (21/799). Dengue virus was earlier considered to be a non-neurotropic virus. 5 However, there are reports describing neurologic involvement in dengue virus infection. 6 Neuroinvasion has been reported in five fatal cases of dengue encephalopathy in which the dengue virus antigen was detected in the brain by immunochemistry. 7
Dengue fever with hypokalaemic quadriparesis has been seen in earlier studies.8,9 The mechanism of hypokalaemia in patients with dengue fever may be due to the redistribution of potassium in cells or transient renal tubular abnormalities leading to increased urinary potassium wasting. 8 All seven dengue fever patients in this series made a dramatic recovery with minimal potassium supplementation compared to the hypokalaemic paralysis of other aetiologies where longer and larger potassium supplementation was needed.
Encephalitis is one of the common manifestations of dengue neurological disease. 10 Encephalopathy is attributed to: cerebral oedema; anoxia; haemorrhage; hyponatraemia; liver or kidney failure; micro capillary haemorrhage; or release of toxic substance.1,10 Cam et al. noted 27 cases of DHF developing encephalopathy. Of these 26 were comatose, 21 had convulsions and one had hemiplegia. No abnormalities were noted on MRI in four of 18 patients with encephalopathy. Other lesions noted on MRI were oedema; scattered focal lesions; cerebral oedema; and, in one, cerebral haemorrhage. 11
Myositis was present in four of our patients. Misra et al. reported five patients presenting with acute pure motor weakness with raised creatinine kinase. 12 EMG and muscle biopsy were consistent with myositis in one of those patients. The pathogenesis of myositis may incriminate myotoxic cytokines, particularly tumour necrosis factor. 13
GBS and ADEM are the immunological manifestations identified in dengue fever. The proposed mechanism for GBS is an antecedent infection evokes an immune response, which in turn can affect the myelin or the axon of peripheral nerve. 14 Both the patients with GBS had recovered completely with conservative management. ADEM following dengue fever has been reported earlier. 15 In ADEM either antiviral antibodies or a cell mediated response to the pathogen may cause cross reaction with the myelin auto antigen resulting in demyelination.
Intracerebral haemorrhage has been postulated as the most common cause of coma in dengue fever patients bleeding from other sites. 16 Siriyakorn et al. reported the first case of dengue with bilateral brachial plexopathy. 17 Although plexopathy has been identified in various viral infection, it is a very rare presentation in dengue infection. One of our patients had lumbar plexopathy.
Mortality rates reported in cases of neurological dengue infection ranged from 5% to 8.35%.1,4,9 Kamath et al. also noted that most neurological events were related to the perfusion status of subjects studied and were found to be the most common cause of death in complicated dengue infections. 4
Limitations of this study included the absence of serological confirmation in nine patients. Dengue IgM ELISA was done after one week of fever. We could not document the same in patients who either succumbed early to the illness or those who had been discharged. However, as these patients presented during an epidemic with the clinical presentation of dengue fever, the diagnosis was not disputed.
Conclusion
Clinicians treating dengue fever should be aware of the varied associated neurological manifestations. In this group of 21 (2.63%) patients who had neurological manifestations, lumbar plexopathy, GBS and ADEM were rare presentations of dengue infection. In patients presenting with quadriparesis, prompt differentiation between GBS and hypokalaemia are critical in management and prognostication.
Footnotes
Acknowledgements
The authors are grateful to Dr Paramdeep Kaur for helping with the statistical analysis.