
Abstract
Medical management of interstitial ectopic pregnancy with high baseline beta-selective human chorionic gonadotrophin (β-hCG) is controversial and there is no consensus on the best treatment option. Here we review the use of methotrexate (MTX) therapy for interstitial ectopic pregnancy, illustrated by three cases in which baseline serum β-hCG levels above 8000 IU/L were successfully managed by systemic MTX therapy. Primary MTX therapy appears to be a promising approach to managing interstitial pregnancy. It offers a safe and effective non-surgical method of treating selected patients even with a high concentration of baseline serum β-hCG. A randomized controlled trial comparing this regimen in interstitial pregnancy with high β-hCG with surgical management is required to substantiate the success and safety of this modality of treatment.
Ectopic pregnancy constitutes one of the leading causes of maternal mortality in the first trimester of pregnancy. 1 Over 10,000 ectopic pregnancies are diagnosed in the UK annually, with an average prevalence of one in 100 pregnancies. 2 Although the incidence of ectopic pregnancy has increased over the last 25 years, fortunately there has been a decrease in the associated mortality. 3 Ten women died as a direct result of ectopic pregnancy over the period 2003–2005 4 compared with 15 women from 1988 to 1990. Maternal mortality has remained largely unchanged at an approximate rate of 0.5–0.6 per 100,000 maternities. 4
The interstitial portion of the fallopian tube is the proximal portion that lies within the muscular wall of the uterus. It is 0.7 mm wide and 10–20 mm long. Interstitial pregnancy represents about 1% of ectopic pregnancies. 5 It is highly morbid with 2.2% maternal mortality due to its characteristic thin myometrium, late presentation and associated massive haemorrhage if rupture occurs. Out of 10 cases of maternal mortality due to ectopic pregnancy in the Confidential Enquiry 2 into maternal deaths 2003–2005, one was interstitial. During the period 2000–2002, there were 11 deaths, of which four were interstitial pregnancies. Interstitial pregnancy poses a significant diagnostic and therapeutic challenge and carries a greater maternal mortality risk than ampullary ectopic pregnancy. They tend to present late (7–12 weeks gestation) due to myometrial distensibility.
Management options include conservative surgical techniques such as laparoscopic cornual resection, laparoscopic cornuostomy or hysteroscopic removal of interstitial ectopic tissue and radical operations such as hysterectomy. 6 Surgical options are associated with an increased risk of severe haemorrhage and emergency hysterectomy. Early diagnosis allows various therapeutic interventions including conservative, medical or surgical management.
Medical management of interstitial pregnancy includes administration of haemabate (carboprost), 7 potassium chloride or methotrexate (MTX), with the latter being most common. Administration could be systemic or local, either ultrasound-guided or laparoscopically, 7–9 referred to as salpingocentesis. Systemic MTX is not operative dependent and is less invasive. There are different regimes for MTX therapy; either single or multiple doses of MTX may be administered using various routes such as oral, intramuscular and intravascular. The most widely used medical treatment at present is intramuscular MTX given as a single dose calculated from patient body surface area (50 mg/m2). For most women this will be between 75 and 90 mg. 10 There are several publications describing successful treatment of all varieties of ectopic pregnancy using a number of MTX regimens. 11–13
Several parameters have been considered as a prerequisite for medical management including the size of the ectopic (<3.5 cm) and baseline serum beta-selective human chorionic gonadotrophin (β-hCG) of <3000 IU/L as recommended by the Royal College of Obstetricians and Gynaecologists (RCOG) 10 and <5000 IU/L by the American Society of Reproductive Medicine. 14 The β-hCG has been identified as an accurate marker of the trophoblastic tissue viability, but the importance of the pretreatment level of β-hCG for the success of therapy is unclear. 15 Some reports 16 indicate that with β-hCG levels above 4000 IU/L the success rate falls to 35% whereas others 17 have reported successful treatment with a level of 38,270 IU/L.
Here we present an unorthodox approach to treatment of interstitial pregnancy by confirming the diagnosis laparoscopically but offered medical treatment with the use of MTX therapy. We provide examples of three case reports of interstitial ectopic pregnancy in which baseline serum β-hCG levels above 8000 IU/L were successfully managed by MTX therapy. High β-hCG in this context refers to levels above 5000 IU/L. 14 Some may find this approach unorthodox. Others may object to the use of laparoscopy for diagnosis that does not proceed to surgical treatment. The recognition that conventional management of interstitial pregnancy has the potential for significant consequences on morbidity and subsequent fertility has influenced our decision to introduce conservative methods as a first line of treatment paralleling the management of standard ectopic pregnancies. We believe this is the first report of diagnosis of interstitial pregnancies using laparoscopy but managed conservatively.
Materials and methods
All our patients were haemodynamically stable, had unruptured ectopic pregnancy, had no pelvic pain and underwent adequate preoperative counselling regarding treatment options for medical and surgical management. They desired future fertility and agreed to comply with regular follow-up, including the use of a reliable contraception for up to three months post-treatment. There was no contraindication to therapy (Table 1) and all patients consented to MTX treatment and follow-up. Patients were counselled regarding treatment options in accordance with RCOG 10 recommendations, including three methods of MTX therapy, and were allowed to opt for any method of their choice.
Contraindications to methotrexate therapy*
*Adapted from the American Society of Reproductive Medicine Guideline 14
Pretreatment investigations, medical management (including single or multiple oral or intramuscular MTX) and follow-up were in accordance with our hospital protocol (Table 2). Ethical approval was not required for our investigation since the method of management to be employed was within a recognized treatment approach at this Trust. The patients gave full consent for their cases to be discussed or presented in meetings and published in a peer-reviewed journal. Treatment was considered successful if there was complete regression of β-hCG and no surgical intervention was required.
Grimsby protocol: single and multiple dose MTX treatment protocol for ectopic pregnancy at Diana Princess of Wales Hospital Grimsby*
MTX, methotrexate; IM, intramuscular; β-hCG, serum beta selective human chorionic gonadotrophin
*Adapted from single-dose protocol of Stovall and Ling 34 and fixed multidose protocol of the American Society of Reproductive Medicine Guideline 14
†Another dose of 50 mg/m2 may be required if β-hCG has not fallen by 15% between days 4 and 7 if patient is systemically well (single-dose protocol)
Case reports
Case 1
A 25-year-old presented with painless vaginal bleeding 12 weeks into her fourth pregnancy. Abdomino-pelvic examination was unremarkable except for slight vaginal bleeding. Her admission serum β-hCG was 10,891 IU/L. A transvaginal ultrasound scan (TVS) showed no evidence of intrauterine gestation and interstitial pregnancy was not positively identified. Diagnostic laparoscopy was performed on suspicion of ectopic pregnancy on account of the β-hCG exceeding our discrimination zone (≥1500 IU/L) and absent evidence of intrauterine gestation. Laparoscopy revealed a large right interstitial pregnancy (Figure 1). Surgical removal was deferred due to potential risk of haemorrhage and hysterectomy until further discussion with the patient. She opted for medical management and received multiple oral MTX as per local hospital protocol.
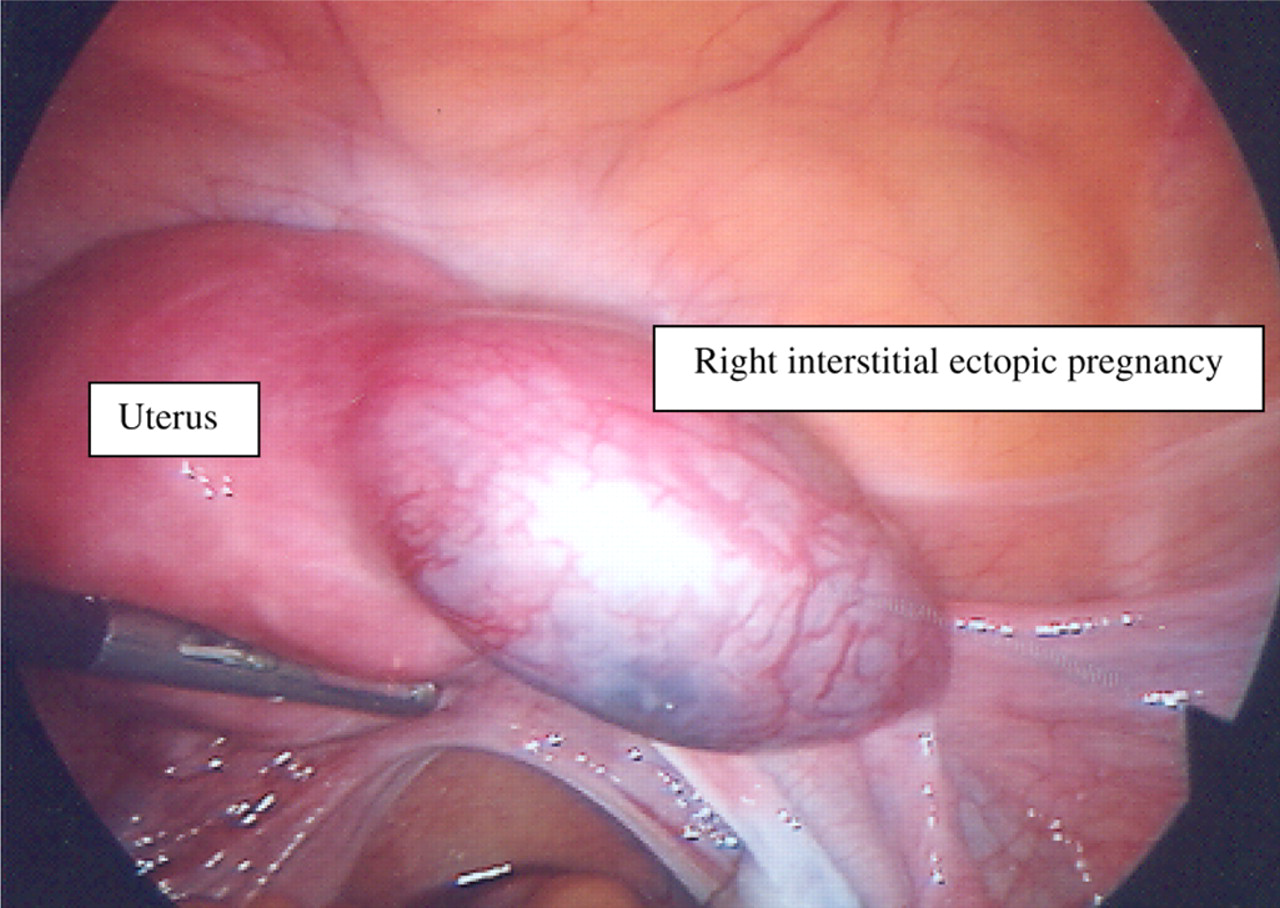
Laparoscopy: right interstitial ectopic pregnancy
TVS performed after laparoscopic diagnosis identified the ectopic pregnancy and was helpful for monitoring its size after treatment. On the fourth day of treatment β-hCG fell to 3033 IU/L. Follow-up investigations were within normal limits. Approximately six weeks later, β-hCG had fallen to just 2 IU/L. At the start of treatment the right interstitial ectopic pregnancy measured 21.0 × 17.0 mm with TVS (Figure 2). At a repeat scan six weeks later, the dimensions were 14.7 × 15.7 mm. At the request of the patient, tubal patency tested by laparoscopy and a dye test at three months post-treatment showed a persistent right cornual ectopic that appeared to be calcified (Figure 3). The left fallopian tube was patent. TVS at six months demonstrated that the ectopic pregnancy had shrunk to 9.0 × 10.0 mm. About a year later, the patient conceived and had a spontaneous full-term normal delivery of a female infant weighing 2740 g.

Coronal transvaginal ultrasound image of a right interstitial ectopic pregnancy; complex cystic mass with an echogenic rim of gestational sac located close to the uterus. The diagnosis of interstitial pregnancy was made by visualization of the interstitial line adjoining the gestational sac and the lateral aspect of the uterine cavity and continuation of the myometrial mantle around the ectopic sac
Laparoscopy and methylene blue tubal instillation three months post-treatment. Persistent right interstitial ectopic pregnancy and patent left fallopian tube
Case 2
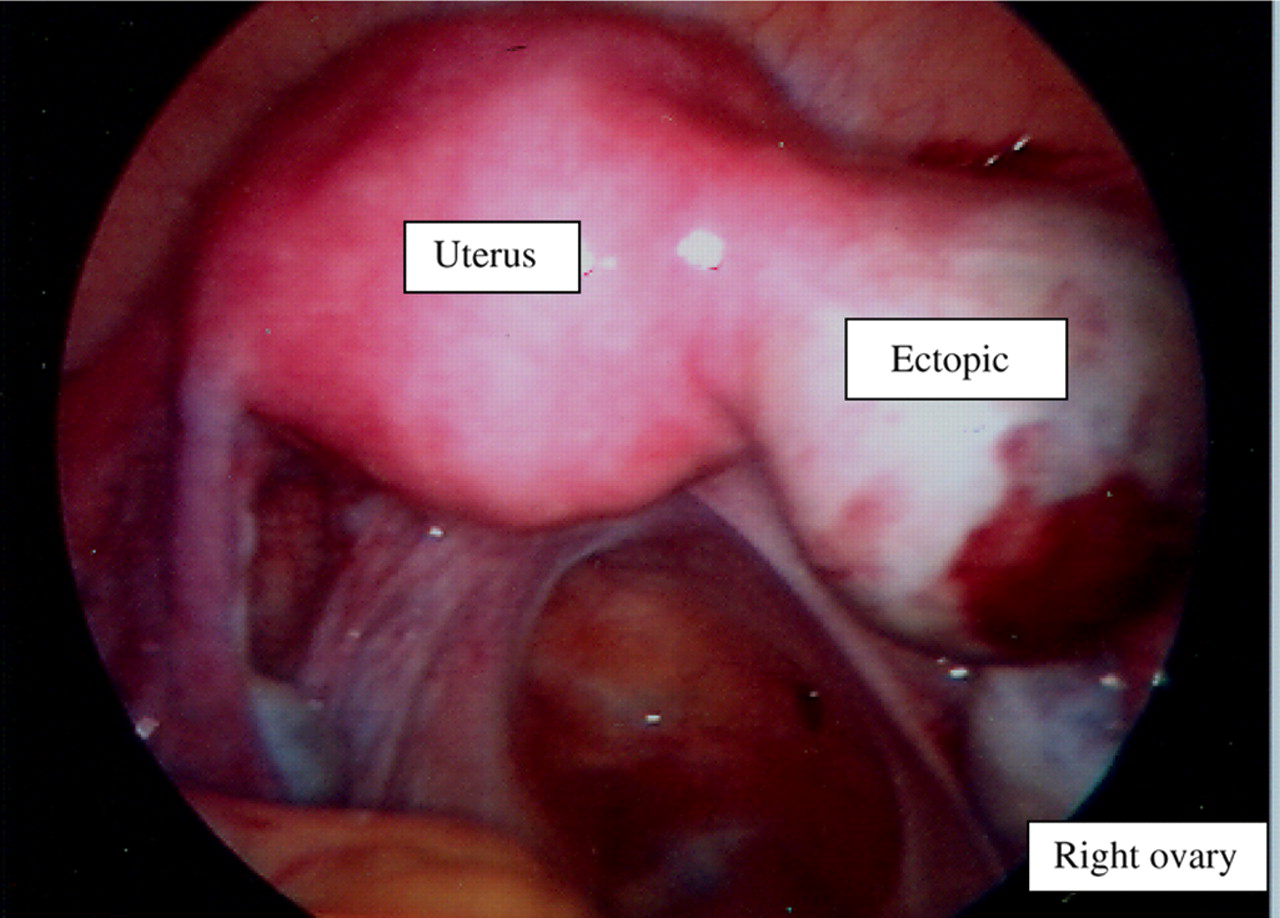
A 27-year-old nulligravida was uncertain of her last menstrual period and was admitted with positive pregnancy test and vaginal bleeding. Her β-hCG was 5921 IU/L. TVS did not positively identify the interstitial ectopic pregnancy but revealed the absence of an intrauterine gestation sac. Her repeat β-hCG 48 hours later was 8206 IU/L. Diagnostic laparoscopy confirmed a left subserous fibroid and left interstitial ectopic pregnancy with no haemoperitoneum (Figure 4a). Surgical treatment was deferred. Following further counselling for therapeutic options, the patient favoured intramuscular multiple dose MTX. Pretreatment and follow-up investigations were within normal limits except for serum β-hCG. It rose to 12,339 IU/L on the fifth day but gradually reduced to 680 IU/L in the fourth week and 1 IU/L in the sixth week. Ultrasonography at one week revealed a 18.3 mm size ectopic, which had increased to 29.3 mm at six weeks (Figure 4b) with gradual reduction to 23 mm in the third month (Figure 4c). Six months later the patient conceived but this pregnancy resulted in early embryonic demise which was managed expectantly. The patient had a complete miscarriage.

(a) Laparoscopy showing left subserous fibroid and left interstitial ectopic pregnancy. (b) Endovaginal scan: left interstitial ectopic pregnancy 6 weeks after treatment (left-right orientation reversed on the scan). (c) Endovaginal scan: left interstitial ectopic pregnancy three months after treatment. Adjacent subserous fibroid (arrowhead) and uterus (double arrowhead)
Case 3
A 35-year-old in her second pregnancy was admitted at seven weeks gestation with vaginal bleeding and right iliac fossa pain that rapidly resolved. She had a past history of pelvic inflammatory disease and her admission β-hCG was 4829 IU/L. Ultrasound showed a 19 mm complex mass in the right adnexum (Figure 5a), which was suspicious of a tubal ectopic pregnancy. There was no free fluid in the pelvis. Diagnostic laparoscopy (Figure 5b) confirmed slight right cornual enlargement with no free fluid in the Pouch of Douglas. The patient was asymptomatic and abdomino-pelvic examination was unremarkable, therefore she opted for conservative management. Her β-hCG was 6332 IU/L at 48 hours increasing to 9572 IU/L at 96 hours. Her β-hCG rose to 16,005 IU/L and the ectopic mass increased to 36 mm at another scan one week after laparoscopy. After further escalating β-hCG levels, the patient changed her mind and opted to receive a single dose of intramuscular MTX.
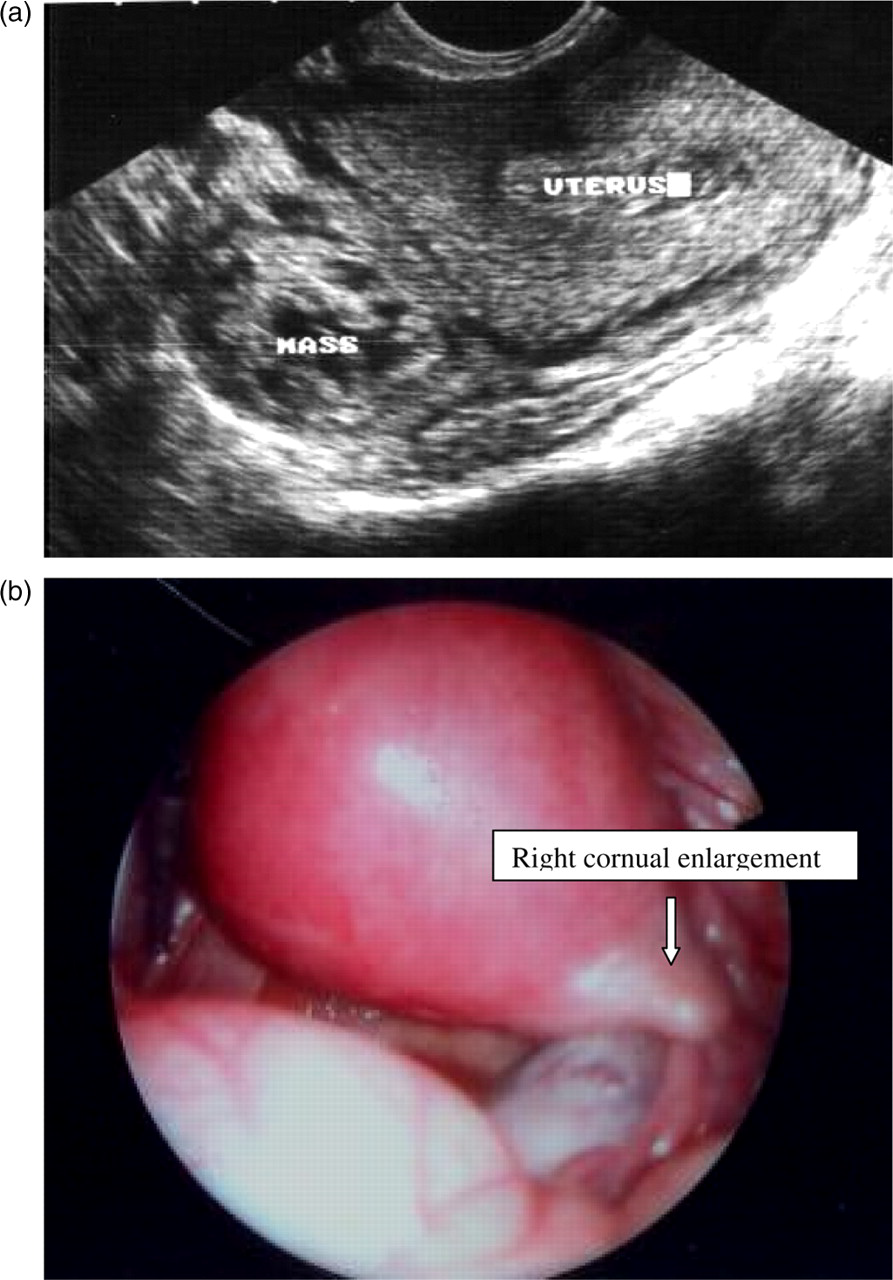
(a) Endovaginal scan: complex mass in the RIF, right iliac fossa. (b) Laparoscopy: slight right cornual enlargement (interstitial ectopic pregnancy)
The MTX was administered at a starting β-hCG of 17,665 IU/L. The level gradually decreased to 16,579 IU/L (day 4), 11,889 IU/L (day 7), 119 IU/L (4 weeks) and to 4 IU/L at 12 weeks post-treatment. The regression of β-hCG for all the three cases is shown in Figure 6. The ectopic mass had reduced to 30 mm at ultrasonography three weeks after treatment, and hysterosalpingography after three months revealed bilateral tubal patency (Figure 7).
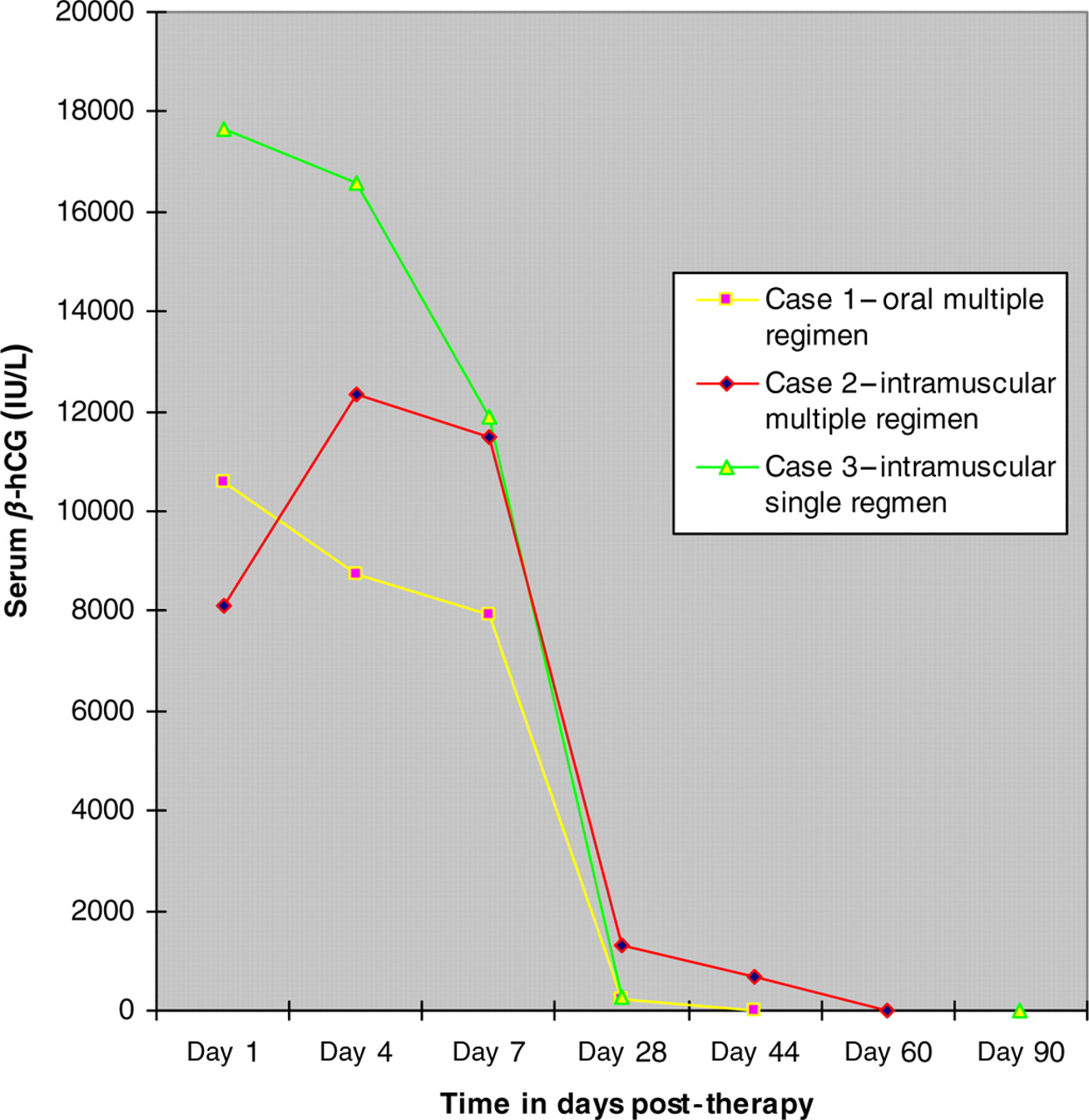
Regression of serum β-hCG after methotrexate therapy in interstitial pregnancy using different regimens
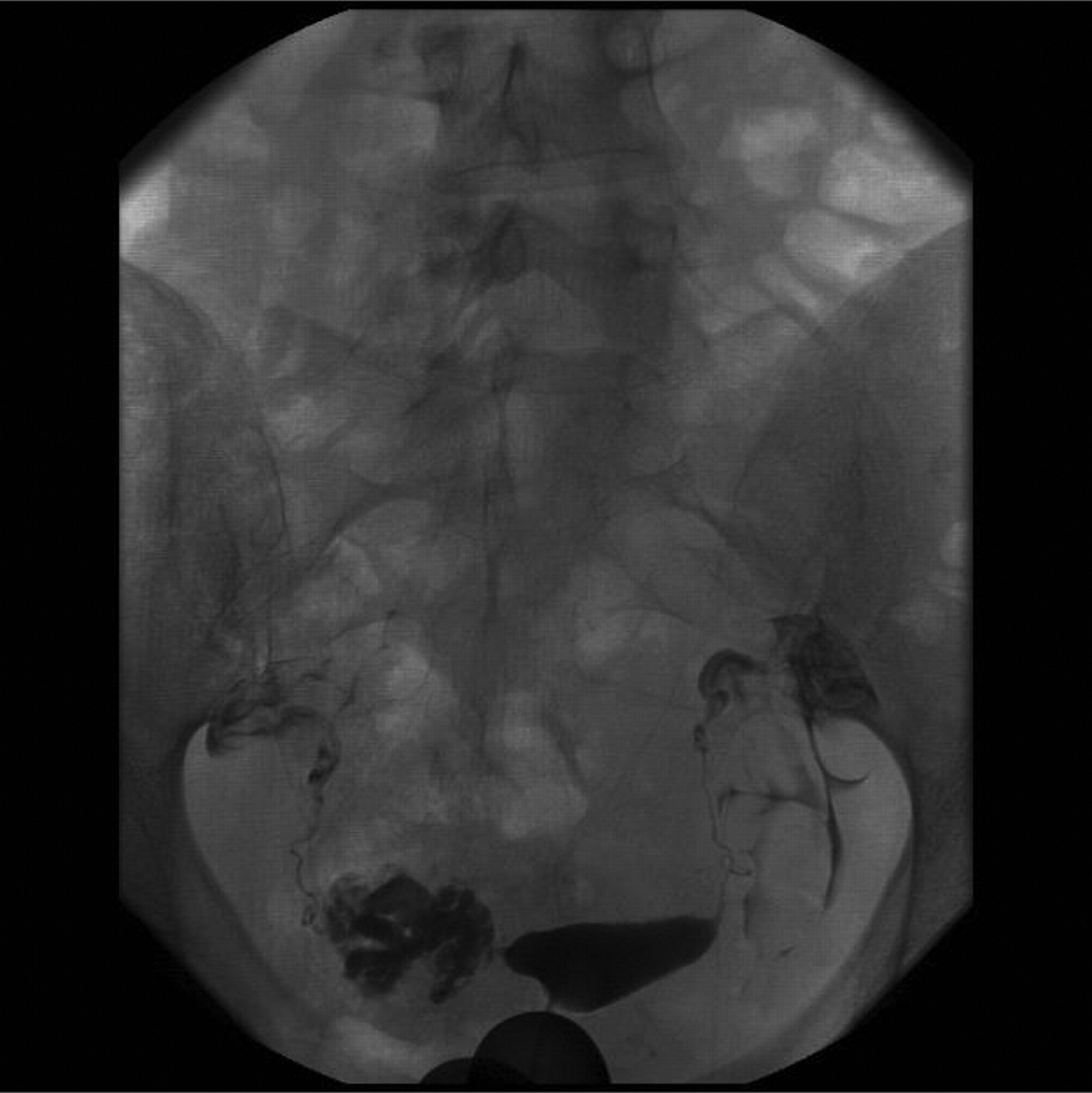
Hysterosalpingogram (HSG): retroverted uterus: normal uterine cavity. Bilaterally patent fallopian tubes with free spill seen bilaterally
Eighteen months later, the patient presented with secondary subfertility. Bilateral tubal blockages were established at a laparoscopic tubal assessment. There were multiple large nodules on the inferior surface of the right liver lobe (Figure 8). Differential diagnoses included MTX toxicity, cystic diseases of the liver, cirrhosis, adenoma, haemangiomatous change, or possibly an amoeboma in view of her previous residence in Gambia. She was referred to the gastroenterology unit for advice. Clinical, biochemical and biophysical assessment in the form of computerized tomography of the liver were all normal. She was referred to a Human Fertilisation and Embryology Authority (HFEA)-licensed tertiary centre for assisted conception.

Nodularity seen on the inferior surface of the right lobe of the liver at laparoscopy and dye test
All three patients were monitored closely at the early pregnancy assessment unit after initial period of stay (5–8 days) in hospital. The regression of serum β-hCG concentration between days 4 and 7 was variable among our patients, as shown in Figure 6. There was a rise in day 5 and suboptimal fall in day 7 for the second case (intramuscular multiple therapy). The percentage change in serum β-hCG between day 4 and 7 for all is shown in Table 3. Table 4 summarizes the treatment regimens and outcome.
Changes in serum β-hCG level after MTX treatment
MTX, methotrexate; IM, intramuscular; IU, international unit; β-hCG, serum beta selective human chorionic gonadotrophin
*Serum β-hCG levels are checked on days 4 and 7 and a further dose is given if β-hCG levels have failed to fall by more than 15% between days 4 and 7
Summary of patients' management and outcome
MTX, methotrexate; CC, complications; IM, intramuscular injection
*Liver nodularity was detected at a post-treatment laparoscopy. Uncertainty remains whether this lesion was present pretreatment
Discussion
The terms cornual and interstitial pregnancies are often used interchangeably, but the two classifications have different ultrasound characteristics. 18 An interstitial ectopic pregnancy is located outside the uterine cavity, within the proximal portion of the fallopian tube, surrounded by a thin layer of myometrium and has communication with the endometrial cavity 18 as described in our cases. A cornual pregnancy on the other hand is a definition that should be reserved only for a pregnancy in the rudimentary horn of a unicornuate uterus.
Ultrasound failed to positively confirm the diagnosis of interstitial ectopic pregnancy in the first two cases before diagnostic laparoscopy. Diagnosis of ectopic pregnancy on TVS should be based on visualization of an adnexal mass or extrauterine gestational sac rather than the absence of an intrauterine gestational sac.
The rate of diagnosis can be improved, however, by interpreting a transabdominal ultrasound scan or TVS using three criteria: an empty uterus, a gestational sac seen separately and <1 cm from the most lateral edge of the uterine cavity, and a thin myometrial layer surrounding the sac. 19
However, the lack of confirmation of interstitial ectopic pregnancy at ultrasonography had no deleterious effect on our patients as there was already enough evidence to reach a diagnosis of ectopic pregnancy. In a prospective study of the transvaginal ultrasound findings of 152 women with suspected ectopic pregnancy who subsequently underwent surgery, over 90% of ectopic pregnancies were visualized by ultrasound prior to surgery. 20 The sensitivity and specificity of transvaginal ultrasonography for detecting ectopic pregnancies were 90.9% and 99.9%, respectively, with positive and negative predictive values of 93.5% and 99.8%, respectively. 21 We have since improved the standard of our ultrasonographic service with dedicated ultrasonographers for obstetrics and gynaecology.
The use of MTX treatment for ectopic pregnancy in patients with high surgical risk factors dates back to the early 1960s and included patients with abdominal pregnancy, with placental attachment to bowel and omentum, 22 interstitial 23 and cervical 24 pregnancies. MTX is an antimetabolite and antifolate drug used in treatment of cancer, medical termination of pregnancy, ectopic pregnancy and autoimmune diseases. It acts as an antifolate by inhibiting enzyme dihydrofolate reductase, which is required for tetrahydrofolate synthesis. Folate is needed for synthesis of DNA, RNA, thymidylates and proteins. Secondary to its effect on high proliferative tissues (e.g. trophoblast), MTX has a strong dose-related potential for toxicity. Side-effects include stomatitis, conjunctivitis, gastroenteritis, impaired liver function, bone marrow depression and photosensitivity.
MTX can be taken orally or administered by injection (intramuscular, intravenous or local). Ectopic treatment success rate by oral use is lower than systemic 25 and there are few reports of these patients being treated with oral MTX, 26,27 intravascular MTX 28 or by local injection into the ectopic site (transvaginal or laparoscopic salpingocentesis). The majority of case series were treated with intramuscular MTX. 29 Some studies 30,31 have suggested that higher β-hCG (>10,000 IU/L) should be considered for multiple dose regimen but there is no clear consensus.
The selection criteria have been changing as experience with MTX for tubal pregnancy has accumulated and monitoring improved. Even the original criteria of Stovall et al. 32 have been modified to include many patients who would initially have been excluded. 33,34 The initial size of the ectopic was limited to <3 cm in early reports. 35,36 This value has steadily increased to the point where size is no longer a major determinant for inclusion. The same is true for the presence of fetal cardiac activity, which is no longer an absolute contraindication to medical treatment. 33,34 The β-hCG concentration is another parameter used to select patients. Although various thresholds have been suggested that are associated with poor outcome, 10,14 many cases have been reported where high β-hCG has been treated successfully with MTX including our report and those of Fisch et al. 37 The latter group reported a case of initial β-hCG of 102,000 mIu/mL and positive fetal cardiac activity. They used a combination of systemic and local injection of MTX.
Surgical treatment for interstitial ectopic pregnancy is associated with increased morbidity, postoperative adhesion or infection. Such treatment involving resection of the interstitium is associated with reduced fertility rates and increased rates of uterine rupture in future pregnancies. 38 Medical treatment, on the other hand, may be associated with a long follow-up, multiple hospital visits (for examinations and investigations such as blood tests), as well as slow shrinkage and disappearance of the ectopic mass. Medical management methods, however, can preserve fertility. Lau et al. 39 concluded that cornual resection or hysterectomy should no longer be the first line of treatment for a haemodynamically stable patient with an interstitial pregnancy.
In this case series of interstitial pregnancies, the baseline serum β-hCG of all patients were above 8000 IU/L. We used MTX in three various regimens, single as well as multiple dose therapy, and we did not give any folinic acid rescue. It is noted that the regression of serum β-hCG was slowest with multiple MTX, fastest with single intramuscular MTX and intermediate with multiple oral therapy.
Our observations support previous suggestions by Lau et al. 39 that this treatment modality can preserve fertility, as demonstrated by two of our cases in which the women became pregnant within months of treatment. A third woman had patent tubes within three months of treatment.
There was no toxicity noted due to MTX in our cases. We were uncertain about the origin of asymptomatic liver nodularity detected two years after treatment at an unrelated investigation in one of the reports. In a previous report, Jermy et al. 40 did not notice any symptomatic or biochemical evidence of toxicity using low-dose MTX without folinic acid rescue.
All of our cases had a successful outcome (β-hCG <5 IU) and pregnancies were achieved spontaneously in two patients within six months to one year after treatment. Prediction of treatment failure either by rising β-hCG or rupture is difficult. Treatment failure has been reported by Lin et al. 41 who described a failed response to a three-dose intramuscular 100 mg MTX treatment (300 mg in total), which was later successfully treated with an ultrasound-guided 100 mg MTX injection. Jermy et al. 40 reported a 94% success in patients treated systemically.
Conclusion
MTX used systemically appears to be a safe option in treatment of unruptured interstitial ectopic pregnancy in patients who are haemodynamically stable, compliant and keen to preserve fertility. Early recognition of interstitial ectopic pregnancy with ultrasound is essential, as only with early diagnosis can conservative therapeutic interventions be maximized. The finding of an empty uterus on ultrasound should always prompt evaluation of ‘the regional triad’ of interstitial, adnexal and the cervical regions.
MTX can be given via an oral or intramuscular route, in single or multiple doses. In our cases we did not use folinic rescue and none of our patients presented with any toxicity. Close monitoring is essential with serial β-hCG tests, ultrasound scans and outpatient medical therapy associated with a saving in treatment cost as well as convenience to patients, especially if primary diagnosis is made by ultrasound.
Appropriate selection criteria for medical therapy remain an important issue and a consensus is required on the predictors of success and failure to optimize management. We recommend that a randomized controlled trial comparing medical treatment for high β-hCG interstitial pregnancy with surgical management be performed to substantiate the success and safety of this modality of treatment.