
Abstract
Hysterosalpingo-contrast-sonography (HyCoSy) is recommended by the National Institute for Health and Clinical Excellence (NICE) as the investigation of choice for otherwise asymptomatic women who need fallopian tube patency assessment as part of their investigation for subfertility. The technique requires the instillation of a positive contrast agent through the cervix, but after the commercial withdrawal of Echovist the only remaining agent, until very recently, was SonoVue, which is not licensed for intrafallopian use. A questionnaire was distributed to 16 units in the UK who were thought to perform HyCoSy in order to collate experience and opinion with this new contrast agent. Eight units replied to say that they had used SonoVue, giving a collective experience of 449 procedures. The opinion would seem to be that results are good and side-effects are rare, making the case to encourage a product licence application. Nevertheless, careful ongoing audit of results is essential and long-term endometrial effects need to be excluded.
The current recommendation from the National Institute of Health and Clinical Excellence (NICE) is that in cases where fallopian tube patency needs to be established, hysterosalpingography, either using X-rays or ultrasound (hysterosalpingo-contrast-ultrasonography or HyCoSy), is the method of choice in otherwise asymptomatic patients. 1 The ultrasound technique requires a positive contrast agent to be instilled through the cervix and until recently the only licensed product for this purpose was Echovist (Bayer plc, Newbury, UK), a supersaturated solution of galactose. Bayer took the commercial decision to remove Echovist (and their other positive contrast agent, Levovist) from the market in September 2009. Hence the only remaining ultrasound positive contrast agent was SonoVue (Bracco SpA, Milan, Italy) and this does not currently have a licence for intrafallopian use.
These events left the units around the UK who had previously relied on HyCoSy for their evaluation of subfertile couples with the options of either abandoning the procedure and resorting to the much more invasive procedure of laparoscopy and dye, or reverting to the use of X-ray hysterosalpingography, or continuing HyCoSy using either a negative contrast agent such as saline or the unlicensed product, SonoVue.
The lack of a product licence is not the only concern about the use of SonoVue for HyCoSy. Its use for echocardiography has been suspended because several patients with pre-existing severe coronary artery disease experienced idiosyncratic hypersensitivity resulting in hypertension, bradycardia and acute myocardial infarction. 2 Its licence currently refers only to its intravenous use for Doppler examinations of liver and breast vasculature. We do not know if SonoVue might have a detrimental effect on either the endometrium or the endosalpinx. There are also physical differences, which may make it more difficult to utilize SonoVue for HyCoSy. It is available only in doses of low volume (5 mL) when reconstituted in sodium chloride solution as per instructions, because it is designed for intravenous injection rather than to fill the uterine cavity. The viscosity of SonoVue is also considerably less than Echovist, giving it a different feel of use. The more viscous product tends to distend the uterus a little before passing down the fallopian tubes whereas the less viscous product travels through the uterus much more quickly and requires continuous low pressure instillation and possibly higher volumes to create the same images. The microbubble stabilizing action of SonoVue is achieved by sulphur hexafluoride rather than galactose, and the echogenic characteristics are different. It is also more expensive.
The primary purpose of this paper is to collate experiences and expert opinions about the use of SonoVue for HyCoSy.
Methodology
In order to establish how units in the UK have responded to the withdrawal of Echovist and to collate experiences and expert opinions about the use of SonoVue, we planned to contact as many units around the UK as possible who we thought might still be offering a HyCoSy service. The authors have organized the only national training programme for HyCoSy for the last 10 years and maintain contact with many previous trainees and hence made use of this database.
All centres around the UK who were recorded on the authors' database and who were thought to be possibly still using HyCoSy were contacted and asked by means of a questionnaire to record their experiences and opinions about the use of alternative ultrasound contrast agents. Sixteen units were contacted. The specific questions are shown in Box 1. Units were also asked for information about their practice and to comment on any difficulties they had encountered.
Questions asked to the nine units that had experience of HyCoSy after the discontinuation of Echovist
Results
Nine of the 16 centres replied. We do not know whether other units did not use HyCoSy or merely declined to answer. Eight had experience of using SonoVue for HyCoSy and four had used saline. The combined experience of the nine units was 3252 examinations performed with Echovist between 1996 and 2009 and 872 procedures subsequently performed with either SonoVue (449 procedures) or saline (423 procedures). Each unit's answers to the questionnaire and some selected comments are given in Table 1. All nine units wished to continue with HyCoSy, rather than resort to either X-ray hysterosalpingography or to routine laparoscopy and dye studies.
Responses to the questionnaire about the use of SonoVue for HyCoSy from the nine centres in the UK
Comments
‘One vial of SonoVue used for 3 or 4 patients’
‘B flow subtraction necessary’
‘Two ampules are too costly’
‘SonoVue is a far better positive contrast medium for HyCoSy’
‘Sonovue is of greater diagnostic value where there is an increased BMI’
‘Need to ensure that correct MI set for capture of microbubbles’
‘One vial used for 2 cases (diluting half a vial with normal saline 10 mls can also be cost effective)’
‘Does not “sparkle” like Echovist, I think this will increase the number of cases when I am unsure about patency’
‘Safety issues with endometrium remain unexplored [with SonoVue]’
In most units the HyCoSies were performed exclusively by ultrasonographers, and where this was the case the lack of a product licence had created a problem with the switch from Echovist to SonoVue. In the past Echovist was commonly administered by ultrasonographers as part of a Patient Group Directive (PGD). However, this system is more complex with a product that is not licensed, such as SonoVue. One unit was able to establish a PGD in association with the NHS Trust's Chief Pharmacist and relevant clinical development committee. Other units used various systems to ensure that a signed prescription was added to every request either at the time the investigation was requested or at the time it was performed. Patient information sheets had been updated to inform patients that the contrast medium was unlicensed, and on at least one occasion a patient had refused the investigation on these grounds.
No patient had required medical intervention because of complications such as cervical shock, bradycardia, severe allergic reaction or severe pain. The consensus view was that SonoVue was generally associated with less patient discomfort. There were a few cases where pain was said to be severe but these were most often due to a difficult cervical catheterization and hence not related to the contrast medium.
The problem of low volume was addressed by a number of units who diluted the SonoVue to varying degrees. In our unit we began by diluting with 10 mL of saline so as to give a similar volume to that previously used with Echovist, but as the average volume of contrast used proved to be only 4.08 mL we now dilute with only 5 mL. If additional contrast is required, for example when pathology is obstructing the view of the tubes and more contrast is required to improve confidence in the diagnosis, a second vial is made up. Some units reported that they had diluted to an even greater volume and hence were able to address the issue of increased cost by using one vial of SonoVue for several patients.
The HyCoSy examination with SonoVue was reported to give as good if not better visualization of the fallopian tubes as Echovist. However, one observation was that the medium did not ‘sparkle’ so much when it moved through the intramural part of the tube and some ultrasonographers thought that this would lead to more cases where they were unsure of tubal patency, and hence increase the false-positive rate of the test. Not surprisingly, there seemed to be a tendency for practitioners to be happier using SonoVue as they gained greater experience with its use.
Discussion
HyCoSy is used as a first-line outpatient investigation to determine the patency of the fallopian tubes in women presenting with infertility. 3 The sensitivity of the test for detecting tubal occlusion is approaching 100%, 4–7 as the appearance of moving contrast in the fallopian tube is characteristic (Figure 1). The specificity is lower, and can be as low as 55%, 7 because it is not always possible to obtain a clear view of the tube or the tube may be in spasm, and hence no flow may be seen in a patent tube. Nevertheless, the technique has been shown to be an excellent screening test to reduce by 75% the use of laparoscopy and dye, hence minimizing the need for a full general anaesthetic and a surgical incision. 8
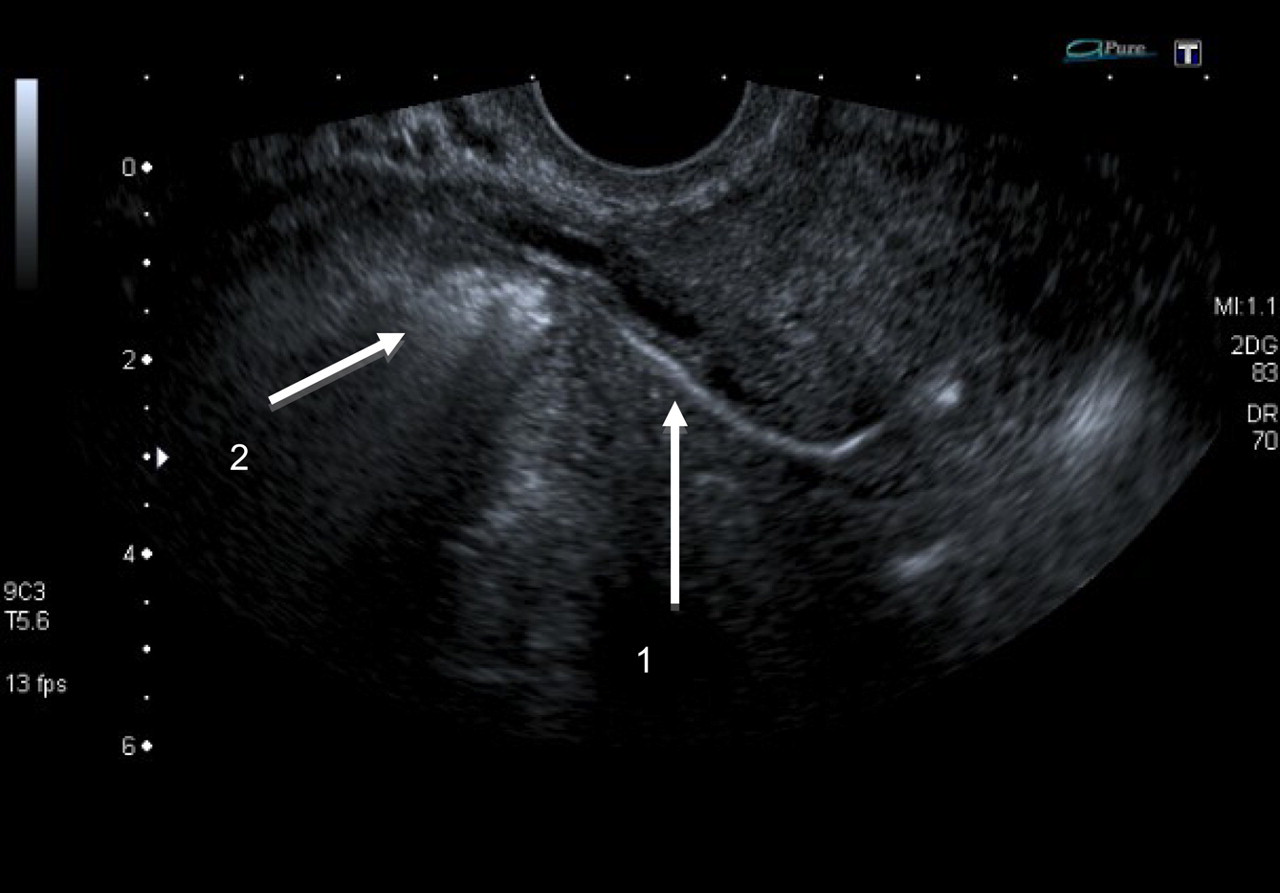
HyCoSy examination showing the positive contrast material SonoVue passing through the right fallopian tube (arrow 1) and spilling from the fimbrial end (arrow 2)
SonoVue is currently marketed throughout Europe and reports exist of its use for HyCoSy in China. 9 Very recently ExEm foam (de Smit Medical Systems Ltd, Bristol, UK) has been introduced onto the market and has a CE mark for intrauterine use, but its performance for HyCoSy is yet to be evaluated.
Examinations are usually performed in the follicular phase of the cycle so as to avoid the possibility of a fertilized oocyte being displaced backwards along the fallopian tube, which might increase the chance of an ectopic implantation. Luteal phase examinations are also associated with a poorer view because of the increased thickness of the endometrium around the tubal ostia. Prescan analgesia in the form of a non-steroidal anti-inflammatory drug is usually given and some units favour prophylactic antibiotics. Complications are rare but include cervical shock following instrumentation of the cervix, severe allergic reaction, pain and acute pelvic infection.
The four units in our study that had tried using saline as a contrast agent all thought the images to be inferior to those obtained when a positive contrast agent was used. This is in agreement with the previously published data. 10 One unit, however, continued to use saline rather than SonoVue because of the lack of long-term safety data, particularly with regard to the effect of sulphur hexafluoride on the endometrium.
We acknowledge the limitations of our study, which should not be viewed as a robust comparison of the effectiveness of SonoVue with other contrast agents, but we believe it represents a valuable overview of current practice within a selection of experienced units within the UK.
Conclusions
Despite the commercial withdrawal of the positive contrast agent, Echovist, many fertility units in the UK are keen to continue with HyCoSy as a way of determining fallopian tube patency and minimizing the use of laparoscopy and dye studies. Practitioners have tried to circumvent a number of problems encountered with the use of SonoVue, which overall seems to be an adequate replacement agent, although concerns about the lack of safety data relating to its long-term effects on the endometrium remain. We believe it would be helpful if SonoVue had a product licence for intrafallopian use and was available in a higher volume vial. The very recent introduction of ExEm foam may prove to be a good alternative. Ongoing clinical audit of the use of SonoVue and other contrast agents for HyCoSy is essential. To this end, we are currently formulating a national online database of HyCoSy procedures to which all HyCoSy practitioners are invited to contribute and receive data.
Footnotes
ACKNOWLEDGEMENTS
The units and individuals involved in this study as members of the UK HyCoSy special interest group: Aarti Umranikar (Southampton University Hospital), Chantal Simonis (Wessex Fertility Ltd, Southampton), Moira Dibb (Victoria Hospital, Blackpool), Suzanne Briggs (South Manchester University Hospitals NHS Trust), Trevor Wing (The Women's Natural Health Practice, Surrey), Collette Coppack (Harrogate District Hospital), Gurjit Rai-Tidbury (Ashford and St Peter's NHS Trust), Maha Ragunath and Fiona Dack (CARE fertility, Nottingham).
DECLARATIONS
The authors have no conflicts of interest to declare.