
Abstract

Part I: Basic Guidelines
Key principles for the safe use of ultrasound
Medical ultrasound imaging should only be used for medical diagnosis. Ultrasound equipment should only be used by people who are fully trained in its safe and proper operation. This requires:
an appreciation of the potential thermal and mechanical bio-effects of ultrasound; a full awareness of equipment settings; an understanding of the effect of machine settings on power levels. Examination times should be kept as short as is necessary to produce a useful diagnostic result. Output levels should be kept as low as is reasonably achievable while producing a useful diagnostic result. The operator should aim to stay within the British Medical Ultrasound Society (BMUS) recommended scan times (especially for obstetric examinations). Scans in pregnancy should not be carried out for the sole purpose of producing souvenir videos or photographs.
Background
Diagnostic ultrasound is an imaging modality that is useful in a wide range of clinical applications, and in particular, prenatal diagnosis. There is, to date, no evidence that diagnostic ultrasound has produced any harm to humans (including the developing fetus).
Despite its apparent excellent safety record, ultrasound imaging involves the deposition of energy in the body, and should only be used for medical diagnosis, with the equipment only being used by people who are fully trained in its safe and proper operation. It is the scan operator who is responsible for controlling the output of the ultrasound equipment. This requires a good knowledge of scanner settings, and an understanding of their effect on potential thermal and mechanical bio-effects.
A fundamental approach to the safe use of diagnostic ultrasound is to use the lowest output power and the shortest scan time consistent with acquiring the required diagnostic information. This is the ALARA principle (i.e. as low as reasonably achievable). It is acknowledged that in some situations it is reasonable to use higher output or longer examination times than in others: for example, the risks of missing a fetal anomaly must be weighed against the risk of harm from potential bio-effects. Consequently, it is essential for operators of ultrasound scanners to be properly trained and fully informed when making decisions of this nature.
The thermal index (TI) and mechanical index (MI) were introduced to provide the operator with an indication of the potential for ultrasound-induced bio-effects. TI provides an on-screen indication of the relative potential for a tissue temperature rise. MI provides an on-screen indication of the relative potential for ultrasound to induce an adverse bio-effect by a non-thermal mechanism such as cavitation. Three forms of the TI may be displayed:
The thermal index for soft tissue (TIS): This is used when ultrasound only insonates soft tissue, as, for example, during obstetric scanning up to 10 weeks after the last menstrual period (LMP); The thermal index for bone (TIB): This is used when the ultrasound beam impinges on bone at or near its focal region, as, for example, in any fetal scan more than 10 weeks after LMP; The thermal index for cranial bone (TIC): This is used when the ultrasound transducer is very close to bone, as, for example, during transcranial scanning of the neonatal skull.
Obstetric examinations
Any potential bio-effects are likely to be of greatest significance in the embryo or fetus. Thus, when undertaking obstetric scans, the restrictions to scanning times detailed in Figure 1 are recommended. These have been formulated on the basis of potential thermal effects arising from the scan, and are therefore based on the TI displayed. MI values should be kept as low as reasonably achievable, consistent with the need to obtain diagnostically satisfactory images. More detail can be found in the Detailed Guidelines.
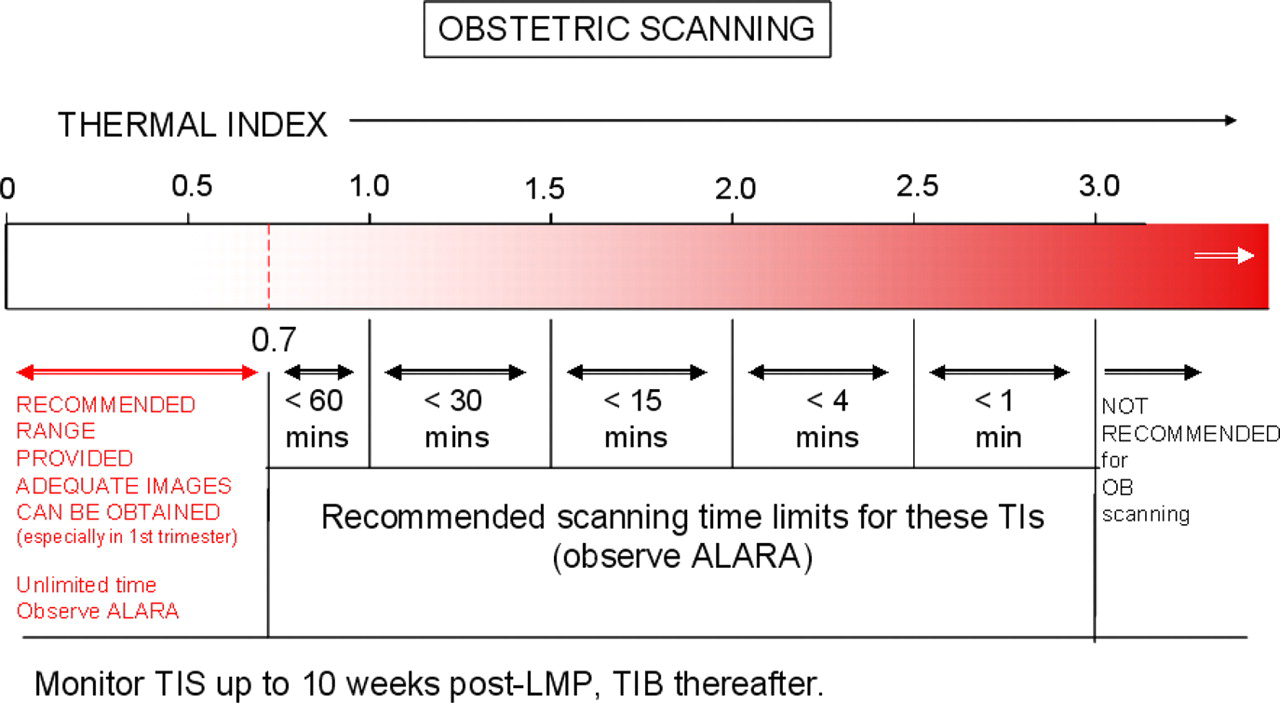
Recommended maximum scanning times for obstetric examinations conducted with different displayed thermal indices (TI). Full information on the recommendations for obstetric and non-obstetric examinations can be found in the Detailed Guidelines
Non-obstetric examinations
Most other types of examination are of less concern than obstetric scans. Specific guidance on a range of non-obstetric examinations (including gynaecological, neonatal, ophthalmic, general abdominal, cardiac, etc.) can be found in the Detailed Guidelines.
Part II: Detailed Guidelines
Scope and purpose
These Detailed Guidelines are intended to assist all those who use diagnostic ultrasound equipment for any purpose in order that they may be able to make informed judgements about ultrasound safety, and in order to protect patients from excessive exposure. These BMUS Detailed Guidelines are based on the best scientific information available at the time of writing, using advice and evidence from international experts. They must be read and understood in conjunction with the BMUS Safety Statement (
Guidelines for probe and system use
Initial power setting
Scanners should be set up so that the default (switch-on) setting of the acoustic output power control is low. If a low default setting cannot be achieved, a low setting should be selected after switching on. A low setting should be selected for each new patient. The output should only be increased during the investigation if this is necessary to produce a satisfactory result.
Exposure time
The overall examination times should be kept as short as is necessary to produce a useful diagnostic result.
Stationary probe
The probe should not be held in a fixed position for any longer than is necessary, and should be removed from the patient whenever there is no need for a realtime image or spectral Doppler acquisition. For example, using the freeze frame or cine loop facilities allows images to be reviewed and discussed without continuing the exposure.
Probe self-heating
Endo-cavitary probes (e.g. vaginal, rectal or oesophageal probes) should not be used if there is noticeable self-heating of the probe when operating in air. This applies to any probe, but particular care should be taken if transvaginal probes are to be used to investigate a pregnancy during the first 10 weeks after LMP.
The raised tissue temperature due to probe self-heating is likely to be greater for endo-probes than for surface probes. This is because the adjacent tissue is at an initial temperature of 37°C, or higher in the case of a febrile patient, rather than closer to room temperature as in the case of surface-applied probes. Also, there is no opportunity for heat removal by air convection or radiation, as is the case for probes applied to the patient's skin. International Standards 2 are intended to limit the maximum temperature of the probe in contact with the patient to 43°C, either internally or externally, or to 50°C when running in air.
Doppler modes
The use of spectral pulsed Doppler, or colour Doppler mode with a narrow write-zoom box selected, is not recommended for the investigation of any of the sensitive tissues identified in the ‘Hazard and risk factors’ section below, unless the user monitors the TI (if available), and performs a risk–benefit analysis. If the TI is not available, the user should find an alternative method of estimating the maximum likely temperature rise.
Pulsed Doppler techniques generally involve greater temporal average intensities and powers than B- or M-mode, and hence greater heating potential, due to the high pulse repetition frequencies and consequent high-duty factors that are often used. In the case of spectral pulsed Doppler, the fact that the beam is held in a fixed position during an observation leads to a further increase in temporal average intensity. Colour flow mapping and Doppler power mapping involve some beam scanning, and so generally have a heating potential that is intermediate between that of B- or M-mode and that of spectral pulsed Doppler.
Hazard and risk factors
Awareness of scanner factors influencing hazard
Operators should understand the likely influence of the scanner controls, the operating mode (e.g. B-mode, colour Doppler imaging or spectral Doppler) and probe frequency on thermal and cavitation hazards.
There are no universal rules for predicting the effect of scanner controls (other than the output power control) on output, since, in an effort to limit outputs, manufacturers often arrange for more than one parameter to change when a particular control is adjusted. However, the following may be helpful as a general guide. In scanning modes, greater heating potential is often associated with multiple or deep transmission focus settings, and the use of write zoom (particularly with a long, narrow or deep zoom box). In spectral pulsed Doppler mode, greater heating potential is usually associated with a high pulse repetition frequency (e.g. a high limit on the frequency scale), and a shallow range gate. The likelihood of cavitation is greater for large output settings and lower frequencies. In Doppler modes, the likelihood is increased by selecting short range gates or by selecting a high Doppler frequency scale.
Sensitive tissues
Particular care should be taken to reduce the risk of thermal hazards when exposing the following to diagnostic ultrasound:
an embryo less than eight weeks after conception; the head, brain or spine of any fetus or neonate; an eye (in a subject of any age).
Up to eight weeks after conception, organogenesis is taking place in the embryo. This is a period when cell damage might lead to fetal anomalies or subtle developmental changes. The brain and spinal chord continue to develop through to the neonatal period.
The presence of bone within the beam greatly increases the likely temperature rise, due to direct absorption in the bone itself and conduction of heat from bone to adjacent tissues. The following table identifies the important relevant landmarks in early pregnancy.
The eye is particularly vulnerable to thermal hazards since the lens and the aqueous and vitreous humours have no cooling blood supply. This applies to an eye of a subject of any age (e.g. child or adult) as well as a fetus, although a fetal eye is better cooled, due to its liquid environment.
Pre-existing temperature elevation
Particular care should be taken to reduce output and minimize exposure time of an embryo or fetus when the temperature of the mother is already elevated.
Thermal and mechanical indices
For scanners which display on-screen TI and MI values, operators should continually monitor their values and use control settings that keep them as low as is consistent with achieving diagnostically useful results. There should be independent checks that the displayed TI and MI values are accurate. These should be made soon after installation and after hardware or software changes.
The MI is an on-screen indicator of the relative potential for ultrasound to induce an adverse bio-effect by a non-thermal mechanism including cavitation.
The MI is intended to offer a rough guide to the likelihood of the occurrence of cavitation. Its value is constantly updated by the scanner, according to the control settings, using the formula
where f is the pulse centre frequency and p − 0.3 is the maximum value of peak negative pressure anywhere in the ultrasound field, measured in water but reduced by an attenuation factor equal to that which would be produced by a medium having an attenuation coefficient of 0.3 dB cm−1 MHz−1.
The TI is an on-screen indicator of the relative potential for a tissue temperature rise.
The TI is intended to give a rough guide to the likely maximum temperature rise that might be produced after long exposure. Three forms of TI may be displayed, depending on the application. TIS assumes that only soft tissue is insonated. TIB assumes bone is present at the depth where the derated temporal average intensity is greatest. TIC assumes bone is very close to the front face of the probe. However, note that errors in calculating TI values, and the limitations of the simple models on which they are based, means that TI values can underestimate the temperature elevation by up to a factor of two.
Application-specific guidelines
For scanners which display TI and MI values on-screen, operators should continually monitor their values and use control settings that keep them as small as is consistent with achieving diagnostically useful results.
Where on-screen MI or TI can be displayed, the recommended exposure times and upper levels for the indices depend on the clinical application. These recommended levels are given in Table 1 for obstetric (including gynaecological examinations when pregnancy is possible) and neonatal ultrasound, and in Table 2 for other applications. Many scanners allow MI and one of the TI values to be displayed simultaneously: the appropriate TI value depends on the clinical application and the recommended indices to monitor are also given in Tables 1 and 2. Graphical representation of the recommended exposure times at different index values for different applications is presented in Appendix A.
Recommended exposure time and index values for obstetric and neonatal ultrasound
TIS, thermal index for soft tissue; TIB, thermal index for bone; TIC, thermal index for cranial bone; LMP, last menstrual period; TI, thermal index; MI, mechanical index
✓ There is no known reason to restrict scanning times in this region
A Many scanners allow MI and one of the TI values to be displayed simultaneously: the most appropriate TI value depends on the clinical application
B TI > 0.7 – the overall exposure time (including pauses) of an embryo or fetus or of the neonatal central nervous system should be restricted
C TI > 1.0 – the overall exposure time (including pauses) of other parts of the neonate should be restricted
D MI > 0.3 – there is a possibility of minor damage to neonatal lung or intestine. If such exposure is necessary, try to reduce the exposure time as much as possible
E MI > 0.7 – there is a risk of cavitation if an ultrasound contrast agent containing gas microspheres is being used. There is a theoretical risk of cavitation without the presence of ultrasound contrast agents. The risk increases with MI values above this threshold
Recommended exposure time and index values for non-obstetric and non-neonatal ultrasound
TIS, thermal index for soft tissue; TIB, thermal index for bone; TIC, thermal index for cranial bone; TI, thermal index; MI, mechanical index
✓ There is no known reason to restrict scanning times in this region
A Many scanners allow MI and one of the TI values to be displayed simultaneously: the most appropriate TI value depends on the clinical application
B TI > 1.0 – the overall exposure time (including pauses) should be restricted
C MI > 0.7 – there is a risk of cavitation if an ultrasound contrast agent containing gas microspheres is being used. There is a theoretical risk of cavitation without the presence of ultrasound contrast agents. The risk increases with MI values above this threshold
D Transcranial ultrasound investigations may require higher acoustic output or longer monitoring times than other applications. When times longer than those recommended here are required, it is recommended that monitoring is paused regularly to minimize exposure
Where an on-screen TI or MI is not displayed, try to obtain
A Medical Physics department may be able to make these estimates, using either a thermal test object or measurements of acoustic power and intensity. For abdominal and obstetric applications, the worst-case estimate of temperature elevation should use a model similar to TIB in which soft tissue overlies bone, with the interface lying at the depth where the de-rated temporal average intensity is a maximum. For other applications (e.g. the eye or superficial bone), the model used should be appropriate to the particular tissues involved.
The operator should aim to stay within BMUS recommended scan times. If there is a clinical need to exceed these recommended times, the ALARA principle should still be followed. When overall times longer than those recommended here are essential, the probe should be removed from the patient whenever possible, to minimize exposure.
TI values are intended to give a rough indication of the likely equilibrium temperature rise that might be produced. However, theoretical 3 and experimental 4 studies have shown that, in some circumstances, TI can underestimate the temperature elevation by a factor of up to two. As a safety precaution, the TI values given in Table 1 are assumed to be half the actual worst-case temperature elevations. Thus, a TI value of 1 is considered to correspond to a worst-case temperature elevation of 2°C.
Following their review of the literature on the effects of temperature elevation on animal fetuses, the World Federation for Ultrasound in Medicine and Biology (WFUMB) 5 concluded that an ultrasound exposure that elevates human embryonic or fetal temperature by 4°C above normal for five minutes should be considered potentially hazardous. Miller and Ziskin 6 showed that there is a logarithmic relationship between temperature elevation and the exposure time needed to produce adverse biological effects in animal fetuses. They showed that, for temperatures below 43°C, the necessary exposure time reduced by a factor of four for every 1°C increase in temperature elevation. Adopting a maximum safe exposure time of four minutes for a temperature elevation of 4°C, and applying the above logarithmic rule, results in the following exposure times:
In Table 1, rounded values of the above exposure times have been used for obstetric exposures up to 15 minutes. The 64 and 256 minute maximum exposure times have been reduced to 30 and 60 minutes, respectively, as a safety precaution to reflect the present lack of knowledge about possible subtle bio-effects associated with prolonged moderate temperature elevation. No time limit is specified for TI values of less than 0.7, in accordance with the statement in the WFUMB 6 recommendations on thermal effects that a diagnostic exposure that produces a maximum temperature rise of no more than 1.5°C above normal physiological levels (37°C) may be used clinically without reservation on thermal grounds.
In examinations of the embryo or fetus in the first eight weeks post conception, when there is no ossified bone, only soft tissue is exposed and so TIS should be monitored. In all other obstetric applications, TIB is recommended as the particular TI value to monitor. This avoids the complication of constantly switching attention between TIS and TIB according to whether or not bone is being insonated, and introduces a safety factor since TIB values are always greater than or equal to TIS values.
To protect the still rapidly developing neonatal central nervous system, the time limits recommended for fetal examinations are also applied to imaging of the brain or spine of a neonate. When imaging other parts of the neonate, the recommended time limits match those for adult tissues.
In eye scanning applications, it is recommended that TIS is monitored as this is the TI used in the study by Herman and Harris, 7 which concluded that, in eye scanning, TIS values should be limited to a maximum of 1.0.
In other applications TIS, TIB or TIC may be monitored depending on the tissue being scanned: in most applications TIB is recommended. The American Institute of Ultrasound in Medicine (AIUM) 8 concluded that there was a maximum safe exposure time for thermal damage to non-fetal tissue, which depended on temperature.
Harm at a particular temperature increase had not been observed for shorter times. In formulating Table 2, we have assumed that TI may underestimate temperature rise by a factor of 2, and we have rounded the maximum exposure times. The 256-minute maximum exposure time has been reduced to 120 minutes as a safety precaution to reflect the present lack of knowledge about possible subtle bio-effects associated with prolonged moderate temperature elevation. As a precaution for transcranial ultrasound, the recommended time limits are the same as those for neonatal brain, except that there is no specific restriction when TIC is less than or equal to 1.0.
The MI value of 0.3, representing the threshold for the possibility of capillary bleeding in gas-containing organs, such as the lungs and intestines, is taken from the 1992 Statement on Non-human Mammalian in vivo Biological Effects of the AIUM. 9
The MI value of 0.7 is chosen as the threshold for cavitation, following the theoretical study by Apfel and Holland, 10 from which the formula for MI is derived. The model used for this study assumes the availability of micro-bubble nuclei of all sizes. Such micro-bubbles are believed to be produced when the shells of the micro-bubbles of some ultrasound contrast agents are destroyed by pulses with higher acoustic pressures. There is experimental evidence that cavitation damage occurs in animals when contrast agents are present. 11,12 In tissues not containing such artificially introduced nuclei, cavitation due to diagnostic ultrasound remains a theoretical possibility only, although it is produced in tissue during lithotripsy treatment 13 and bubble formation has been demonstrated in agar gel exposed to diagnostic levels of ultrasound. 14