
Abstract
The aim of this study was to investigate a number of issues involving UK shoulder surgeons' use of ultrasound. We surveyed members of the British Elbow and Shoulder Society by inviting them to complete a questionnaire. Data collected included the incidence of the use of shoulder ultrasound in clinic, indications for ultrasound, the experience and training undertaken by those performing the scan, and source of funding for equipment.
The use of ultrasound in the orthopaedic outpatient department as a diagnostic/management tool for the shoulder surgeon is increasing in popularity and has even been described as an essential adjunct in the diagnosis of rotator-cuff pathology. 1,2 Proponents of ultrasound argue that its use allows diagnosis of shoulder conditions in the clinic, allows the formation of a surgical plan at the initial consultation given that the operator can correlate examination findings to radiological findings, and allows patients to better understand the diagnosis/disease pathology. 1,3 It is non-invasive and cost-effective with machines available from as little as £5000. 3 This increase in popularity may also reflect the relatively poor sensitivity and specificity of orthopaedic clinical examination particularly in the detection of partial tears of the rotator cuff. 4
Furthermore, several papers have reported that orthopaedic surgeons are capable of demonstrating near equal accuracy in the diagnosis of full-thickness rotator cuff tear as radiologists. 5
Ultrasound is recognized as the most operator dependent of the imaging modalities, and has been described as an art, implying it can be difficult to acquire the necessary skills to reach an acceptable and reproducible standard. 6 This then raises concern over training, competency and issues of clinical governance when ultrasound is to be used by an individual surgeon. The Royal College of Radiologists (RCR) recommends that in order to attain competence, surgeons should attend a course on the theory of ultrasound including aspects of physics, safety, ultrasound techniques, image recording and filing. Further training should involve attendance at one clinic per week for three to six months supervised by a grade 2 ultrasound practitioner, with a minimum of 250 examinations recorded in a logbook and a competency assessment. 7
Other issues surrounding the use of ultrasound by non-radiologists in general include the loss of an independent assessment of pathology, the potential for deskilling radiologists and ultrasonographers, the inability of cheaper machines to record the ultrasound images for future reference or issues of governance. 3 Additionally, the purchase of an ultrasound machine for use by an individual clinician may not represent an efficient use of resources. 3
With the perceived increasing trend within the shoulder surgical fraternity towards the routine use of shoulder ultrasound in the clinic and the increased publication bias in the medical literature towards papers that advocate the routine use of shoulder ultrasound, the time was right to conduct a survey. The survey was designed to establish:
the current uptake of shoulder ultrasound among shoulder surgeons in the UK clinical indications for conducting their own scans level of training and experience source of funding for machines.
Methods
Surgeons in the UK who were members of the British Elbow and Shoulder Society (BESS) were surveyed using an anonymous, four-page, reply-paid questionnaire. The questionnaire was designed by using the co-authors' combined knowledge of the use of shoulder ultrasound among shoulder surgeons.
The questionnaire sought information about each surgeon's place of work (district general hospital/teaching hospital/specialist shoulder centre/private hospital), number of consultant surgeons in his/her unit and whether the surgeon used ultrasound to examine the shoulder routinely during the clinic.
For those using ultrasound in clinic they were asked open questions regarding:
Indications for ultrasound The nature of training and experience with ultrasound and funding used to purchase the machine. Indications for outpatient ultrasound and who performs it Intention to take up routine shoulder ultrasound in the clinic Previous use of shoulder ultrasound in clinic.
For those NOT using ultrasound in clinic they were asked about their:
We analysed replies to the questionnaire using Microsoft Access to construct frequency tables.
Results
Of the 360 questionnaires distributed, 89 (25%) were returned; 86 could be used in the analysis. Of those returned, the three not used were because one surgeon was retired, one surgeon operates exclusively on elbows and one surgeon returned the questionnaire blank. All results presented are based on the 86 responses.
Surgeons worked in a variety of settings: 14% in specialist centres, 58% in district general hospitals, 26% in teaching hospitals and 2% in private practice exclusively. Some 20% of surgeons worked as a lone shoulder surgeon in their unit, while 37% were one of two surgeons and 27% were one of three surgeons in their unit.
The results were intended to be analysed by categorizing survey respondents into two groups: those using ultrasound during clinic and those who were not. However, during the analysis a third group emerged – consultants who had radiology support during clinic time to perform ultrasound scans when requested. With this in mind the respondents were split into three groups rather than the two as originally planned.
Almost a quarter (23% n = 20) of surgeons used ultrasound routinely during the clinic, 9% (8) of surgeons had radiology support available in terms of a musculoskeletal (6) or general radiologist/ultrasonographer (2) available to perform shoulder ultrasound if needed during clinic hours. The majority (67% n = 58) of surgeons did not use ultrasound routinely in the clinic. A significant number of respondents (22%) intended to use ultrasound in their practice at some point in the future.
Table 1 demonstrates the demographics of each of the groups in terms of place of work and number of consultants in each unit.
Demographics of each of the groups in terms of place of work and number of consultants in each unit
USS, ultrasound scanning; OPD, outpatient department
The main indications given (Table 2/Figure 1) for shoulder ultrasound were (1) to confirm a diagnosis of rotator cuff tear for all surgeons, (2) to determine the size of the tear for 70%, (3) impingement in 40%. There were more indications given by surgeons who use routine shoulder ultrasound (performed by themselves or a radiologist), including biceps tendon pathology, calcific tendonitis and for assistance in intra-articular injection compared with those surgeons who did not use ultrasound in clinic.
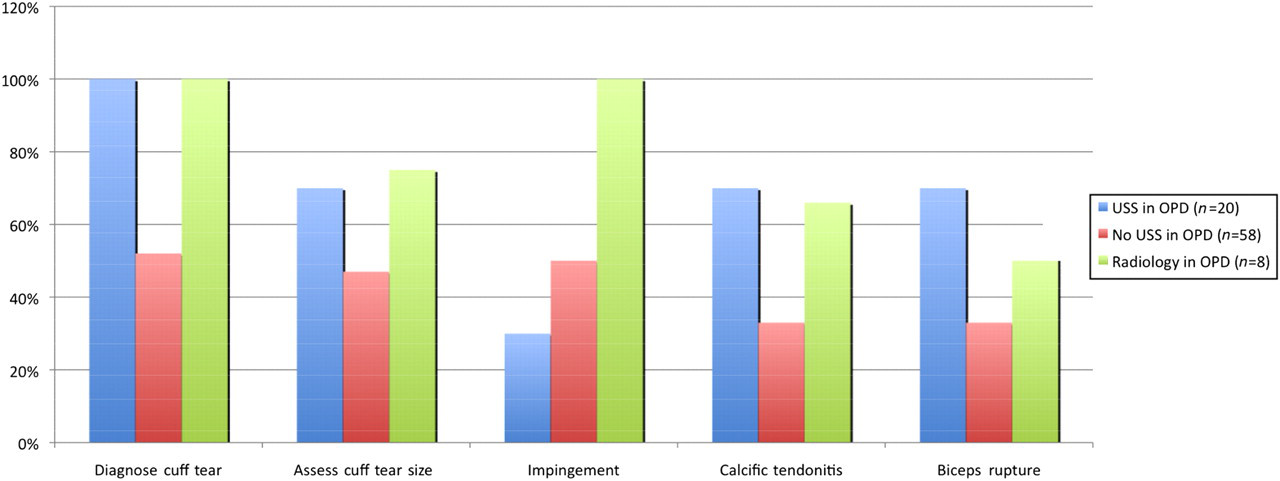
Frequency of indications for ultrasound per surgeon group
Main indications for ultrasound per consultant group
Table 3 demonstrates the training, experience and funding of surgeons using shoulder ultrasound. The most common method of training was by a short course, most surgeons using ultrasound being established in practice and having performed more than 200 ultrasound procedures in their overall experience. There was a mix of funding resources, with more than two-thirds of machines financed by the surgeons rather than the NHS. One surgeon used the machine based in the operating theatre for assisting the anaesthetist in performing regional blocks.
Training, funding and experience of surgeons using ultrasound
Table 4 demonstrates the reasons for stopping for those who have previously used shoulder ultrasound and the reasons why other surgeons intend to start practising shoulder ultrasound. Five surgeons felt that ultrasound was not reliable and therefore abandoned it, while others had stopped due to the time the procedure took during the clinic, and one surgeon was concerned over the training required to safely practise shoulder ultrasound. Of those who were intending to commence shoulder ultrasound the majority cited their reason as the advantage of obtaining a quick result from the investigation. However, one surgeon specifically stipulated that he felt obliged to start an ultrasound service in clinic to prevent litigation, given the papers in the medical literature now published advocating its role.
Surgeons used ultrasound previously and intended to use in the future: reasons for stopping and intention to start
Discussion
This study was developed in order to determine the current and possible future use of routine outpatient ultrasound by shoulder surgeons in the UK. Some 20% of responders were currently using ultrasound in clinical practice with a further 22% of those not using ultrasound currently, stating that they were planning to use ultrasound in their practice. The benefits stated were consistent with those stated in the literature; for example, speed of diagnosis, confirmation of cuff tear/size, formation of a surgical plan at the clinic especially in order to reduce waiting times to definitive surgery. These figures indicate that there is a significant level of interest and activity in the use of shoulder ultrasound. These findings thereby raise pertinent questions regarding adequacy of training and issues of clinical governance.
The overall trend for the use of ultrasound in clinic is primarily towards the detection of rotator cuff tears, and secondarily to detect the cuff tear size. Some surgeons also use ultrasound to detect biceps pathology and calcific tendonitis. Given one of the main indications for shoulder ultrasound is to confirm the diagnosis of impingement, as function of the rotator cuff is ‘dynamically’ visualized during the investigation, fewer surgeons than expected used ultrasound to detect impingement. Of interest, those whose ultrasound service was provided by a radiologist used it more frequently for all the above pathologies, especially impingement. This may indicate that surgeons are less confident than radiologists at diagnosing impingement.
However, there is also a group of 12% of surgeons not using ultrasound currently who have used ultrasound in the past. Reasons given for stopping routine use of ultrasound included lack of operator reliability and concern regarding governance. There is some evidence to suggest that ultrasound lacks accuracy for the detection of partial cuff tears compared with full tears in the hands of the orthopaedic surgeon. 5 Additionally, ultrasound cannot assess fatty infiltration of the rotator cuff, information which is required to determine whether functional recovery can be made after cuff repair. In such cases, magnetic resonance imaging would be required. 2
Of those surgeons responding to the survey, none had stipulated that they had completed the necessary RCR requirements to practise shoulder ultrasound. The most popular method of training undertaken was a short course, followed by exposure on a shoulder surgery fellowship. The exact details of the short courses attended were not recorded. Inadequate completion of training could explain why the NHS has only purchased a limited number of machines. In our survey, one shoulder surgeon broke his anonymity over the issue, when he claimed he had been denied funding for an ultrasound machine as the radiology department had blocked its purchase given the surgeon had not completed the necessary training as stipulated by the RCR.
The increasing popularity of ultrasound among shoulder surgeons and the lack of completion of the necessary training requirements to perform outpatient ultrasound demonstrated in this study have important ramifications in terms of governance and patient safety. We raise the question that if surgeons have not completed the required training as stipulated by the RCR, do they place themselves at risk in case of diagnostic error?
It has been acknowledged that the current training requirements for teaching musculoskeletal ultrasound are time-consuming for the busy clinician and the resources for teaching ultrasound skills are limited. 3,6,8 This could explain why surgeons are not completing the recommended training. Increasing the level of resources available for training could increase compliance with the current RCR standards. However, this study may suggest that the RCR requirements are not a respected standard for training or accreditation in ultrasound for shoulder surgeons currently in practice in the UK, as no one individual surveyed has completed this training. On this basis, it would seem to be sensible to conclude that urgent development of new standards that are more realistic in terms of achievement and resource application may be required, in order to deliver a quality service in the interests of patient safety. There are two possible models for the development of guidance for this purpose. The first model was developed in the related specialty of rheumatology. In response to a similar problem of standards required for the accreditation of training for musculoskeletal ultrasound, the European League Against Rheumatism in 2001 developed its own guidelines for basic competency in ultrasound for rheumatologists. 6 In terms of shoulder surgeons this guidance could come from the specialties' own society – BESS, or the British Orthopaedic Association (BOA) for example. The second model that could be applied would involve the RCR working alongside BESS or the BOA to develop training resources, appropriate and realistic standards and/or guidelines acceptable to both stakeholders, acknowledging the role of ultrasound specific to shoulder surgeons. To enable this, the RCR must be mindful that surgeons are different: (1) they are able to validate their scan findings intraoperatively and (2) they perform ultrasound to answer a particular diagnostic question. Any proposed standards/guidelines for training should reflect this, and not be based on those current training requirements for radiologists or ultrasonographers. If guidelines are formed without this important consideration, the danger is that the collaboration could be unsuccessful and unworkable, or the BESS/BOA could be forced into the first model, as suggested, with no input from the RCR.
These suggestions for change in this study are based on a survey response rate of 25%; while previously this may have been thought to be a limitation of the study, more recently the positive association between response rates and survey quality has been questioned. 9
The demographics of the respondents' workplace seems to reflect the distribution of shoulder surgeons, so this sample may be regarded as representative of those in the UK as a whole. An explanation for a non-response in this study could be a lack of willingness by those actively using ultrasound to admit that they are doing so having not completed the current standards for training.
The authors accept that establishing new standards for training would take time to devise and implement. However in both the shorter and longer term, an alternative method of providing a one-stop shoulder ultrasound clinic is for shoulder surgeons to combine resources where available with an established musculoskeletal radiologist or ultrasonographer. This collaboration can be under local arrangement depending on available resources, or could be potentially encouraged through any guidance developed by the RCR and/or BESS/BOA. Some surgeons in this study have gone down this route and are therefore able to combine the advantages of ultrasound in clinic with improved diagnostic capability, while avoiding governance issues related to training and finance issues related to equipment purchase.
In summary, this study has demonstrated that there is significant interest in ultrasound among shoulder surgeons in the UK for use in outpatient departments; no surgeon surveyed had completed the current training requirement for its use as a non-radiologist, and therefore we conclude that for the purposes of governance and quality in practice there is an urgent need for a new set of training requirements that are safe, realistic, specific to the shoulder surgeon and are appropriately resourced.
DECLARATIONS
The authors have no conflicts of interest to declare.