
Abstract
There is perhaps no greater challenge to the emergency and critical care physician than management of the hypotensive patient. A rapid, yet accurate, assessment is essential in this clinical setting. Point-of-care ultrasound (PoCUS) has evolved to become an indispensable test in the critical care and emergency setting. This article addresses the use of ultrasound in the evaluation of the hypotensive patient and reviews some of the scanning protocols and algorithms that have been described. We use the mnemonic FAST and RELIABLE to describe key aspects of PoCUS for undifferentiated hypotension.
Question
Among patients presenting to the emergency department with undifferentiated hypotension, how can I use point-of-care ultrasound (PoCUS) to identify the cause of the hypotension and optimize management?
Introduction
There is perhaps no greater challenge to the emergency and critical care physician than management of the hypotensive patient. These patients are critically ill, and we as physicians sometimes have only minutes to find the cause of the hypotension and treat it correctly before the patient decompensates. This life-threatening situation is made even more difficult by virtue of the fact that the patient is often too unstable to travel for traditional diagnostics such as computed tomography scan, and too sick to wait for results of other radiological or laboratory investigations. Commensurate with the difficulty in diagnosing and managing these patients are the tremendous rewards when you are able to identify and correct the underlying cause and literally save the patient's life. It is indeed this that draws many emergency and critical care physicians to the field.
Point-of-care ultrasound (PoCUS) has evolved to become an indispensable test in the critical care and emergency setting. The many important advantages of ultrasound are:
readily available at the bedside, eliminating the need for travel to unmonitored areas of the hospital; rapid, giving immediate realtime answers to the clinician performing the exam; reproducible, for monitoring response to treatment; inexpensive; free of ionizing radiation; versatile, being able to rule in and exclude multiple different diagnoses.
It is this versatility that makes ultrasound the ideal imaging modality in the evaluation of the critically ill patient with undifferentiated hypotension. Multiple aetiologies of hypotension can be considered and investigated, all with the same machine, in a matter of minutes. The limitation, as with many aspects of the physical exam and other bedside tests, is that ultrasound is operator dependent. Confidence and competence in both image acquisition and image interpretation are essential, as is the knowledge of how to incorporate findings into patient care. This article will address the use of ultrasound in the evaluation of the hypotensive patient and review some of the scanning protocols and algorithms that have been described.
Case example
An elderly man is brought into the emergency department by Emergency Medical Services after being found unresponsive. On examination he is obtunded, localizes pain and moans. His blood pressure is 60/36 mmHg, heart rate is 135 beats per minute (bpm), temperature is 38.3°C, respiratory rate is 36 breaths per minute and SpO2 is 94% on room air. The remainder of the physical examination is significant for thready radial pulses, diffuse mild tenderness and guarding on abdominal palpation, bilateral pitting oedema in the lower extremities, and a fistula for haemodialysis in his left arm. It is difficult to hear his heart or lungs because of his moaning. Lung excursion is diminished bilaterally with coarse upper airway sounds.
As he is intubated and resuscitation is initiated, the cause of his hypotension is sought: Is he septic? Is he dehydrated or fluid overloaded? Does he have cardiac tamponade or a pulmonary embolism? Does he have an abdominal aortic aneurysm (AAA) or a tension pneumothorax? Does he need fluids, antibiotics, blood products or vasopressors? Does he require chest decompression or pericardiocentesis? Should the surgeon be called to have the patient taken to the operating room?
In this critical scenario, is there any FAST and RELIABLE way to sort through these diagnoses and management options? Can PoCUS provide a FAST and RELIABLE approach…?
The examination
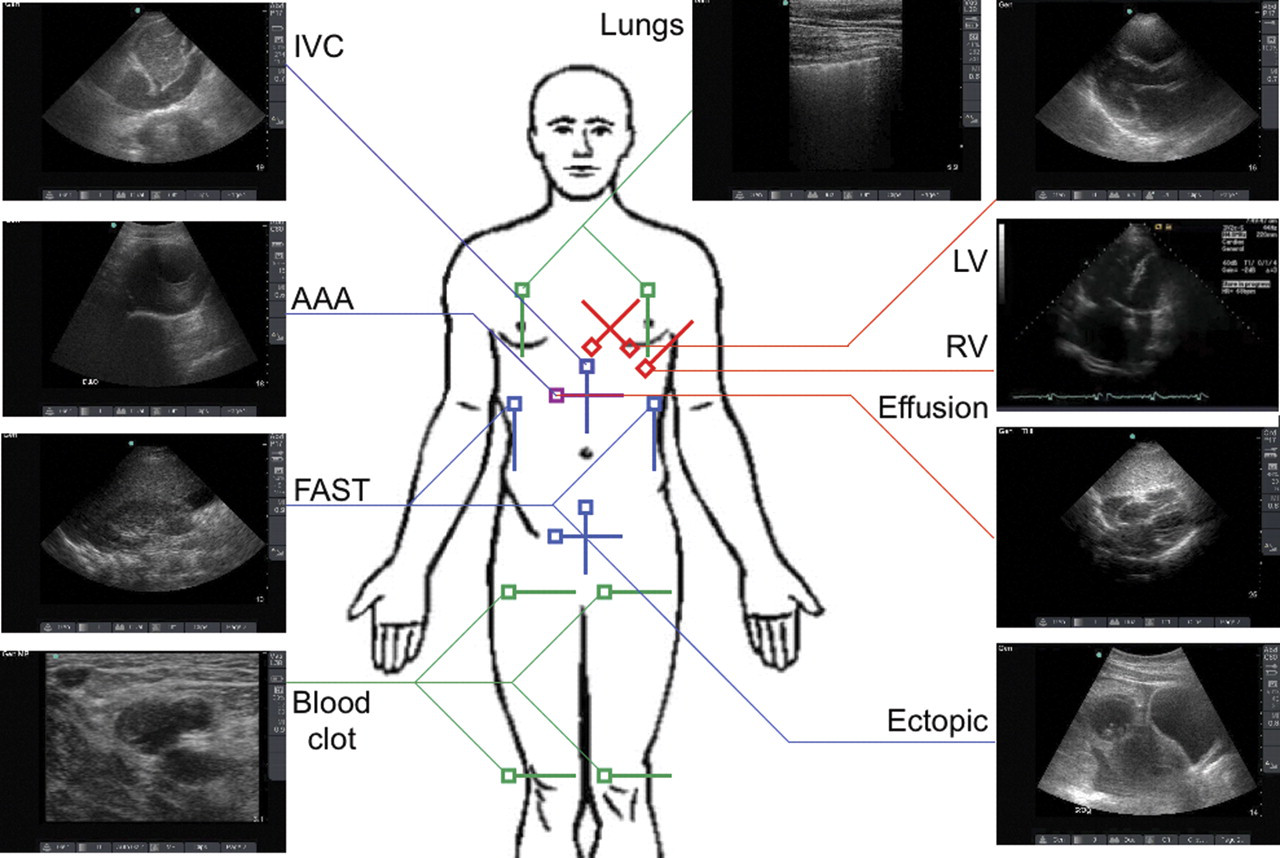
The use of ultrasound in the hypotensive patient is not one unique application, but rather a combination of different PoCUS techniques involving the heart, abdomen, chest and vessels. Several protocols have been described and are summarized below. Each involves a slightly different scanning protocol and evaluates for different pathologies. The authors propose a new protocol, FAST and RELIABLE, which combines many of the applications described in this series, is more comprehensive than most previously described protocols, and serves as a mnemonic for ease of use. Figure 1 depicts the transducer location and orientation for each of these views.
FAST (Focused Assessment with Sonography in Trauma): A standard three-view (right upper quadrant, left upper quadrant, pelvis) scan of the abdomen and lung bases looking for free fluid. When free fluid is seen in the abdomen, the possibility of acute haemorrhage (i.e. from hepatic or splenic injury, ruptured aorta and ruptured ectopic pregnancy) needs to be considered. These may require surgical intervention.
1
Large pleural effusions are also easily identified on the FAST examination if the pleural recesses are visualized. In fact, ultrasound is a more sensitive diagnostic test for pleural effusion than the supine chest X-ray.
2
The presence of pleural fluid can indicate the presence of intrathoracic haemorrhage, oesophageal rupture, cardiac failure or malignancy.
Right ventricular (RV) strain: Best seen on an apical four-chamber view, the ventricular sizes can be compared. When there is an acute pressure overload on the RV as seen with a pulmonary embolism, the RV will dilate and appear larger than the left ventricle. In the unstable patient, thrombolysis (or thrombectomy if there are contraindications) should be considered.
3
Effusion, pericardial: Best seen on the subxyphoid or apical four-chamber views (though any cardiac view may suffice); circumferential fluid around the heart raises concern for possible tamponade. As more fluid accumulates in the pericardial space, the pressure rises and the right side of the heart has difficulty filling completely during diastole. The RV free wall is unable to expand completely and can appear inverted with downward concavity. This is sometimes referred to as ‘scalloping.’ In the setting of persistent hypotension and cardiovascular collapse, emergent pericardiocentesis or a surgical pericardial window is indicated.
Left ventricular (LV) function: Best assessed on the para-sternal long or short-axis view, but any cardiac view may suffice. Determining how strongly the LV is beating is one of the most important uses of ultrasound in the hypotensive patient. No mathematical measurements or calculations are necessary – simple visual estimation has been shown to be as accurate.
4
This is especially true when it is considered that an exact ejection fraction is not needed, but rather stratification into normal (>50%), decreased (30–50%), or severely decreased (<30%) groups. Severely decreased LV function may prompt the need for cardiac inotropes, whereas normal function means that cardiogenic shock can be ruled out. Sepsis can present with any degree of LV function, but in one study a ‘hyperdynamic’ (>55%) LV had been shown to be 94% specific for sepsis.
5
The degree of filling of the LV can also guide fluid management; an underfilled LV is likely to respond to intravenous fluids whereas a dilated LV may not.
Inferior vena cava (IVC): A sagittal or transverse view in the subxyphoid area allows for visualization of the IVC as it crosses the diaphragm and enters the right atrium. The IVC can be used to assess intravascular volume status. Normally, as a person inspires, the negative intrathoracic pressure that is generated facilitates return of blood to the heart, and the IVC collapses. The degree of collapse is related to the central venous pressure, as is the absolute diameter of the IVC. In general, when the IVC is narrow (<1.5 cm) and collapses a large amount (>50%), the central venous pressure is low, a hypovolaemic (dehydration, haemorrhage) or distributive (sepsis, anaphylaxis) cause is likely, and volume resuscitation should be initiated. When the IVC is dilated and non-collapsing, volume depletion is unlikely. A dilated IVC can also be seen in tension pneumothorax, cardiac tamponade, RV infarction, right-sided congestive heart failure or a pulmonary embolism.
6
Aorta: A transverse sweep down the abdomen from the subxyphoid process to the umbilicus with the curvilinear transducer should suffice for interrogation of the aorta. A longitudinal (sagittal) view can also be helpful, and a measurement of the aorta in largest diameter taken. When the aorta is >3 cm, an AAA exists, and in the hypotensive patient, aortic rupture must be kept high on the differential diagnosis (the risk increases with increasing aortic diameter). Free abdominal fluid, either seen on the FAST exam or adjacent to the aorta is highly suspicious for a ruptured aorta, but in general ultrasound's ability to distinguish between ruptured and non-ruptured aortas is very poor. Emergent surgical evaluation and preparation for operative repair are critical.
7
Blood clot, venous (deep venous thrombosis, DVT): Simple compression with a linear transducer of bilateral femoral and popliteal veins can assess for a DVT. In the transverse plane, veins are compressed with downward pressure to the point where the lumen is obliterated. If the anterior and posterior walls fail to touch, a DVT is presumed. The femoral vein should be compressed from the point of take off of the greater saphenous vein to the bifurcation into the superficial and deep femoral veins. While a DVT alone should not cause hypotension, the finding of a DVT in a patient with hypotension of unknown aetiology raises the concern for a pulmonary embolism and in the critically ill hypotensive patient, thrombolysis could be considered on this finding, particularly if seen in conjunction with a dilated RV (see (2)).
8
Lungs – pneumothorax: A curvilinear or linear transducer placed in sagittal orientation on the anterior chest wall in the mid-clavicular line can be used to assess for pneumothorax. The pleural line is visualized immediately inferior to the ribs, and assessed for horizontal sliding. When no sliding is present, a pneumothorax is very likely, and in the setting of a hypotensive patient, needle decompression of the chest should be considered.
9
Ectopic pregnancy: Sagittal and transverse views of the uterus and adnexae in the suprapubic area are used to look for free abdominal fluid, and the presence or absence of an intrauterine pregnancy. If a patient is known to be eight or more weeks pregnant and no IUP is seen, the concern for an ectopic pregnancy is raised. While an empty uterus is not diagnostic of an ectopic pregnancy of less than eight weeks, in the setting of hypotension in a young woman with a postive β-human chorionic gonadotropin, this diagnosis should be suspected and immediate gynaecological consultation must be sought. If a formal transvaginal ultrasound examination is available, visualization of adnexal masses or free fluid will also raise the suspicion for this potentially lethal diagnosis.
10
Transducer location and orientation for each of the components of FAST and RELIABLE. Cardiac, curvilinear and linear transducers are marked with red, blue and green lines, respectively. FAST, Focused Assessment with Sonography in Trauma
This protocol, though lengthier than most, will leave almost no stone unturned in the search for the cause of hypotension. Of the causes of hypotension, almost each one has some finding on ultrasound that can help support or refute it as the aetiology (Figure 2). The physician–sonographer needs to remember that first and foremost he or she is a physician and should appropriately adopt the protocol to the clinical setting (i.e. a scan for AAA will be as useless in a young woman as one for an ectopic in an elderly man.) Though not studied in its feasibility or on its effect on outcomes, the FAST and RELIABLE protocol has the unique advantage of serving as its own mnemonic, which should make it easier to learn and apply.
The causes of hypotension and their ultrasound findings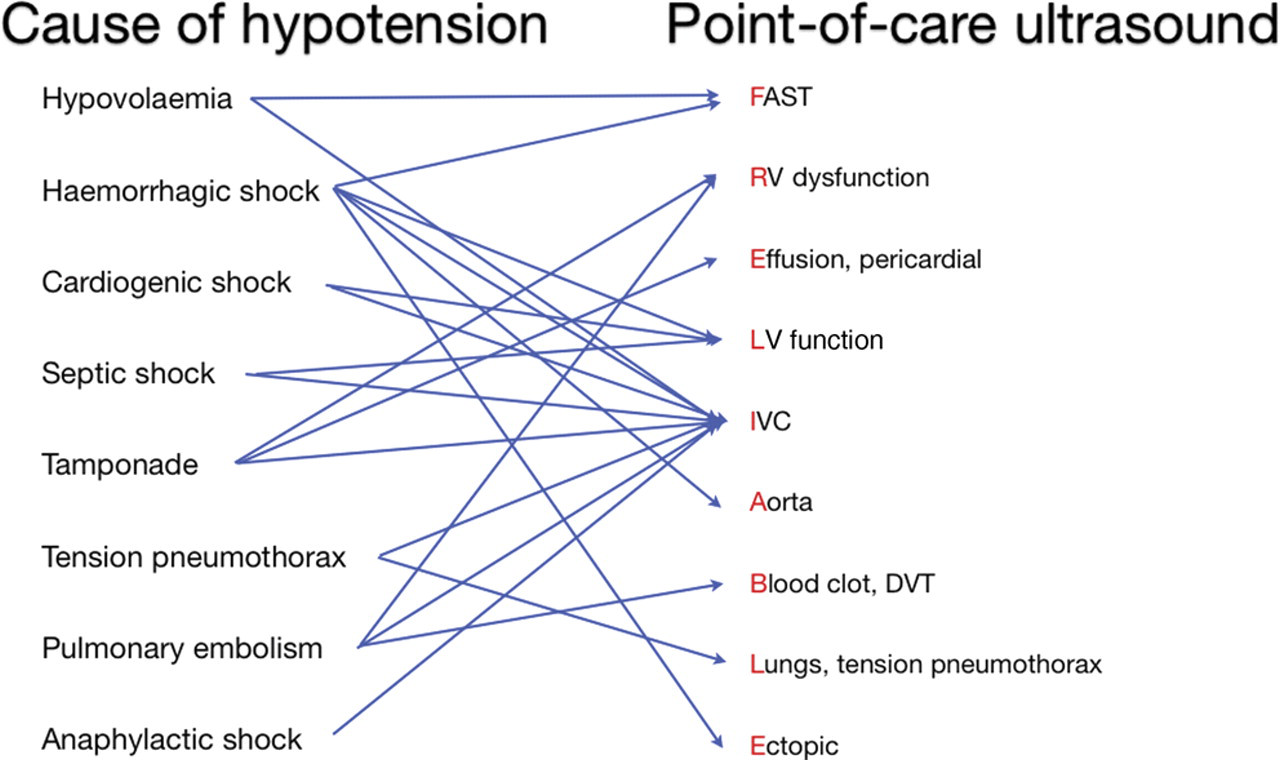
Evidence
The use of PoCUS for undifferentiated hypotension has been well described over the last decade. Most papers are descriptions of techniques; few look at outcomes or effect on management. The most notable are discussed here.
One of the first studies to describe an ultrasound-based protocol for the hypotensive patient was the UHP (Undifferentiated Hypotensive Patient) ultrasound protocol by Rose et al. 11 in 2001. The authors propose a unified scanning protocol looking for free abdominal fluid (single view of Morrison's pouch), qualitative assessment of the heart (single subxyphoid or parasternal view) and AAA (transverse sweep of the length of the aorta). They suggest that the purpose of such a protocol is to have a ‘standardized ultrasound approach to the undifferentiated hypotensive patient that allows for the systematic evaluation of reversible and time-dependent cause of hypotension’. One of the underlying principles of this algorithm that the authors stress is that even though in general single views of structures may be inadequate to definitively rule out pathology, since the patient is hypotensive, any abnormality significant enough to cause this hypotension should be ‘readily detected’.
A randomized, controlled trial of immediate versus delayed goal-directed ultrasound by Jones et al. 12 in 2004 looked at the effect of ultrasound in the management of non-traumatic hypotension in emergency department patients. Two groups were randomized to receive a goal-directed ultrasound at time 0–15 minutes (early) or at 15–30 minutes (delayed), in addition to standard of care. The goal-directed ultrasound consisted of seven views: subcostal cardiac, IVC, parasternal long-axis cardiac, apical four-chamber cardiac, hepatorenal recess, pelvis and rectovesical area, and abdominal aorta, consistently performed in that order. At the 15-minute time point, treating physicians were asked to choose potential causes of the hypotension from a list of 21 diagnoses. The median number of diagnoses at 15 minutes in the group which received early ultrasound was four compared with nine in the group that received delayed ultrasound. Additionally, the correct diagnosis as defined by the criterion gold standard was more often included on the list in the early group (80%) than in the delayed group (50%). While the results of this study do not prove that ultrasound improves patient care, they do show that physicians are better able to identify causes of hypotension, and do so more rapidly. In the setting of the golden hour, where time is of the essence, it is not a large leap to extrapolate that this could ultimately result in better patient care and outcomes.
Much of the rest of existing literature regarding the use of ultrasound for hypotension, shock or cardiac arrest focuses on description of techniques and proposed algorithms. The CAUSE (Cardiac Arrest Ultra-Sound Exam) paper by Hernandez et al. 13 in 2008 describes a protocol designed to identify the most common and reversible causes of cardiac arrest, notably cardiac tamponade, hypovolaemia, pulmonary embolism and tension pneumothorax. They propose an algorithm incorporating a four-chamber echocardiogram and bilateral views of the lungs to rule out each of these causes and suggest that future research in this area could ‘reduce the time required for emergency providers to determine the aetiology of a cardiac arrest and thus decrease the time between arrest and appropriate therapy’.
The ACES (Abdominal and Cardiac Evaluation with Sonography in Shock) protocol was proposed by Atkinson et al. 14 in 2009. The aim of the protocol is to provide a structured approach to ultrasound in hypotension, requiring only an introductory level of training (Level 1/Core applications). It describes a structured six-view scan involving a (1) cardiac view, (2) IVC view, (3) abdominal aorta view, (4) right and (5) left flank view for intra-abdominal and pleural fluid, and (6) a pelvic view for free fluid as a helpful adjunct to clinical examination. The addition of lung and venous windows for pneumothorax and DVT are advised where considered appropriate. The authors suggest that a randomized trial is needed to investigate the protocol's validity in improving management of hypotensive patients.
In a review of ultrasound for hypotension in 2010, Perera et al. 15 described the RUSH (Rapid Ultrasound in Shock) examination. Using a plumbing analogy, it categorizes the causes of hypotension as relating to the pump, the tank, or the pipes. The ‘pump’ exam involves ultrasound of the heart looking for left ventricular function, pericardial tamponade and RV strain. The ‘tank’ examination begins with the IVC to assess intravascular status, then continues to the chest to check for pleural effusions, pneumothorax, pulmonary oedema and then to the abdomen where free fluid can be identified. Lastly the ‘pipes’ examination looks for aortic dissection or aneurysm, and at the legs for a DVT. The paper provides a comprehensive overview of the causes and aetiologies of hypotension and ‘presents the most detailed shock algorithm for use by emergency physicians to date’.
Components of protocols for hypotension
RV, right ventricle; LV, left ventricle; IVC, inferior vena cava; DVT, deep venous thrombosis; X=standard component of protocol; (x)=optional component of protocol
Conclusion
PoCUS has a tremendous role in the care of the patient with undifferentiated hypotension. Within minutes it can definitively identify or exclude multiple possible causes of hypotension and help guide management decisions. FAST and RELIABLE is a comprehensive ultrasound protocol aimed to quickly differentiate between the major causes of hypotension. Although more research is needed to quantify the impact of such a protocol on outcomes, the evidence for the individual components of these protocols is strong. Appropriate training for the use of PoCUS in undifferentiated hypotension provides emergency physicians with a powerful diagnostic tool and should form part of the standard training for all physicians dealing with this patient group.
DECLARATIONS