
Abstract
Introduction
Placing a bare metal stent within the superficial femoral artery (SFA) can prolong vessel patency when compared with balloon angioplasty alone. Subsequent in-stent re-stenosis does occur in some individuals. In our institution, a surveillance programme to identify and treat ‘clinically silent’ stenoses has been running for two years and the purpose of this study was to evaluate this programme.
Methods
Retrospective review of cases was performed making note of indication for stenting, initial clinical outcome and the results of follow-up diagnostic and interventional radiological procedures.
Results
In total, 41 patients were included in the study. The majority (76%) had a good clinical outcome maintained during the first year at which stage a surveillance ultrasound was performed. Sixteen of these showed no evidence of significant in-stent stenosis or occlusion. Eleven of the remainder had ‘clinically silent’ in-stent stenosis. Nine of these had successful in-stent angioplasty. Ten (24%) patients became symptomatic within the first year. Ultrasound in seven of these patients revealed two in-stent occlusions, one in-stent re-stenosis and four with no significant findings. One patient went straight to have angiography, revealing in-stent re-stenosis.
Conclusion
Our surveillance programme has successfully identified and treated clinically silent in-stent stenoses in 22% of patients with an SFA stent who may have progressed to symptomatic stenosis or occlusion. Our results highlight the importance of ultrasound surveillance following stent placement. Based on only one asymptomatic patient experiencing stent occlusion at one year, and symptomatic stent problems occurring anywhere from six to 193 days, we consider that one year surveillance is acceptable.
Lower limb peripheral arterial disease (PAD) is a common, important manifestation of systemic atherosclerosis. It occurs in 3–10% of the population, increasing to 15–20% in people over 70 years of age. 1,2 The most common site of PAD is the superficial femoral artery (SFA). While most patients with PAD are asymptomatic, many have intermittent claudication, chronic critical limb ischaemia or present as an emergency with acute critical limb ischaemia. As a result, PAD significantly impairs quality of life and is the most common cause of lower limb amputation in the western world. 3
Treatment of SFA disease is usually dependent on the length of the lesion. For lesions less than 10 cm long in symptomatic patients, the most common treatment is percutaneous transluminal angioplasty (PTA). While PTA can result in initial technical success rates of more than 95%, late clinical failure remains an important concern with large studies showing the primary patency after PTA in the SFA was 33% in one year. 3
The search for improved patency and clinical results after angioplasty has led to the use of stents in the SFA. Bare metal stents have been utilized in an effort to decrease clinically significant re-stenosis, by increasing the postprocedural vessel luminal diameter. 4 Although primary patency is improved by a stent, there is still a significant re-stenosis rate and this can be detected early by ultrasound and treated with angioplasty. 5
Following an initial audit performed within the department in March 2008, in which in-stent stenosis was seen in 15% of patients with bare metal SFA stents, an ultrasound surveillance programme was implemented with the intention of identifying stenosis prior to symptomatic decline.
Classically, stenting has been reserved for patients with poor angiographic outcome after angioplasty, over 30% residual stenosis following angioplasty, or flow limiting dissection. The ABSOLUTE trial 5 compared outcomes in patients who were randomized between angioplasty and primary SFA stenting at a single centre. The re-stenosis rate (defined as greater than 50% reduction in lumen) in the stented SFA at 12 months was 37%. In the RESILIENT trial, 6 a multicentre randomized trial between PTA and stenting of the SFA, stented patients had a primary patency of 80% at one year. At 24 months, patients who underwent primary stenting had higher clinical success and freedom from target lesion revascularization than patients who underwent balloon angioplasty. Primary patency, assessed for 12 months with ultrasound, was significantly better in the stented group. 6 This audit is retrospective and its aim is to establish whether a scan at one year is the optimum time to pick up in-stent stenosis. We used the ABSOLUTE 5 and RESILIENT 6 trials as a benchmark with which to compare our results.
Methods
Patient selection
All patients on the ultrasound surveillance programme who had undergone endovascular interventions for SFA disease, with placement of one or more stents within the SFA or popliteal artery between May 2008 and April 2010, were retrospectively identified. Any patients who died or were lost to follow-up were excluded from the final statistical analysis.
Vascular interventional procedure
At the initial procedure, all patients underwent balloon angioplasty, followed by placement of at least one self-expanding bare metal stent. Indication for stent placement included suboptimal result following angioplasty and recurrent stenosis within the same segment of SFA. Lesion length varied between 2 and 20 cm, and up to three stents were used across any single lesion. Two different stents were used – Lifestent Flexstar (Edwards Lifesciences, Irvine, CA, USA) and Cordis SMART™ CONTROL™ Stent System (Johnson & Johnson Gateway®, New Brunswick, NJ, USA). These were implanted with the intention of covering the entire diseased segment and to include areas of iatrogenic dissection or intentional subintimal angioplasty. During the procedure, 3000 IU intra-arterial heparin was administered and following the procedure the patient was prescribed dual antiplatelet therapy comprising long-term aspirin 75 mg daily and three months of Clopidogrel 75 mg daily after an initial loading dose of 600 mg.
Postprocedural assessment
Patients were re-assessed clinically within three months of the procedure by their referring vascular surgeon, and thereafter according to clinical need. Approximately 12 months following their procedure, patients attended the ultrasound department for a complete arterial examination of the treated limb. Based on the ultrasound result, if a significant stenosis was detected, angiography with a view to angioplasty was performed, otherwise the patients returned to clinical follow-up with no further planned ultrasound surveillance.
Data collection
The clinical outcomes were obtained from vascular outpatient clinic letters (via the hospital Core Patient Database) and results of imaging were obtained from the radiology department Picture Archiving and Communication System (PACS). The data were maintained in a de-identified database; with these being retrospective data, individual informed consent was not required. The authors sought and obtained local clinical governance approval (Project no.1621) for performing and presenting the data as an audit.
Definitions
Loss of primary patency was said to have occurred for either occlusion or a diameter decrease of at least 50%, based on peak systolic velocity ratio measurements (PSVR), as described below.
‘Clinically silent’ is a term used for patients in whom an asymptomatic but radiologically significant stenosis is identified.
Ultrasound measurements
Ultrasound scans were performed and reported by sonographers who hold the Diploma in Medical Ultrasound (DMU) or Postgraduate Diploma (PgDip) in medical ultrasound in conjunction with either a Postgraduate Certificate (PgCert) in peripheral vascular ultrasound or extensive vascular experience. One of four identical Philips iU22 scanners (Phillips Medical Systems, Best, Netherlands) was used with a 9 MHz linear transducer maintaining a 60° insonation angle, or angle correction when not possible. The common femoral artery (CFA), the femoral bifurcation and the entire SFA, as well as the popliteal artery, were examined in two-dimensional greyscale and with colour Doppler. Peak systolic velocities (PSV) were measured in each artery and throughout the stent. If a stenosis was identified (in-stent or elsewhere), the next most proximal area of normal calibre vessel was used to determine the increase in velocity. The highest PSV within the stent was recorded. PSVR was calculated by dividing the PSV within the stent by the PSV within the proximal disease-free segment. Ultrasound criteria for significant stenosis were taken as doubling of the flow velocity, compared with the proximal adjacent normal calibre segment (PSVR >2).
Results
In total, 41 patients were included in the study. Median (range) age at time of stent placement was 68 (43−90) years.
Asymptomatic patients
Most (76%, n = 31) patients had a good clinical outcome at surgical follow-up appointments during the first year, evidenced by a reduction in symptoms of claudication, rest pain or tissue loss. Surveillance ultrasound scan at one year showed 16 of these patients (39%) had no evidence of significant in-stent re-stenosis or occlusion. A further 11 patients (27%) had ‘clinically silent’ in-stent stenosis, nine of whom went on to have successful angioplasty. Only one was lost to follow-up and one declined a subsequent angiography examination.
Symptomatic patients
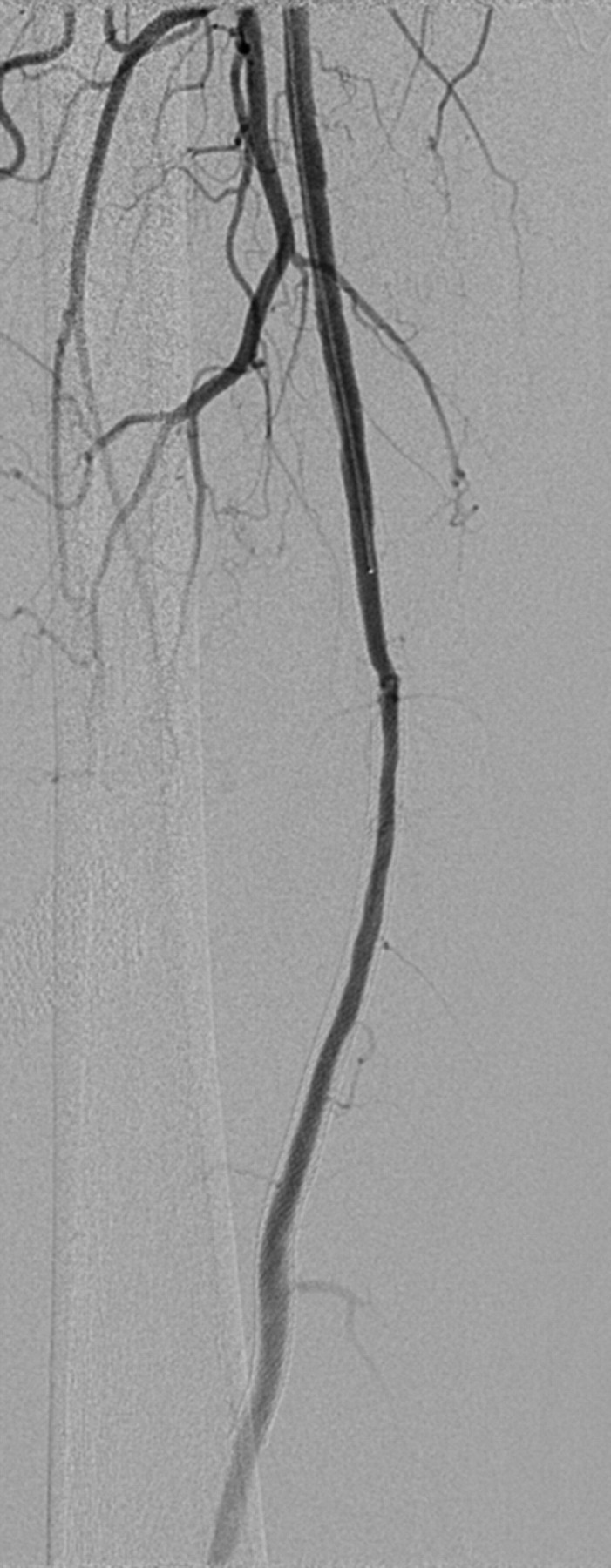
Just under a quarter (24%, n = 10) of patients became symptomatic within the first year, with a return to preprocedural symptoms or worsening claudication/rest pain/tissue loss. Ultrasound in seven of these patients revealed two in-stent occlusions (such as Figure 1), one in-stent re-stenosis (such as Figure 2) and four with no significant findings. One patient went straight to having angiography, revealing an in-stent re-stenosis (such as Figure 3). The median (range) of time between stent placement and symptomatic stenosis or occlusion in the above four patients was 131 (6−193) days.
Colour Duplex image demonstrating occluded proximal SFA stent with patency of profunda femoris Colour Duplex image demonstrating in-stent re-stenosis evidenced by narrowed lumen and increased peak systolic velocity (PSV) Digital subtraction angiogram demonstrating superficial femoral artery patency but with diffuse in-stent re-stenosis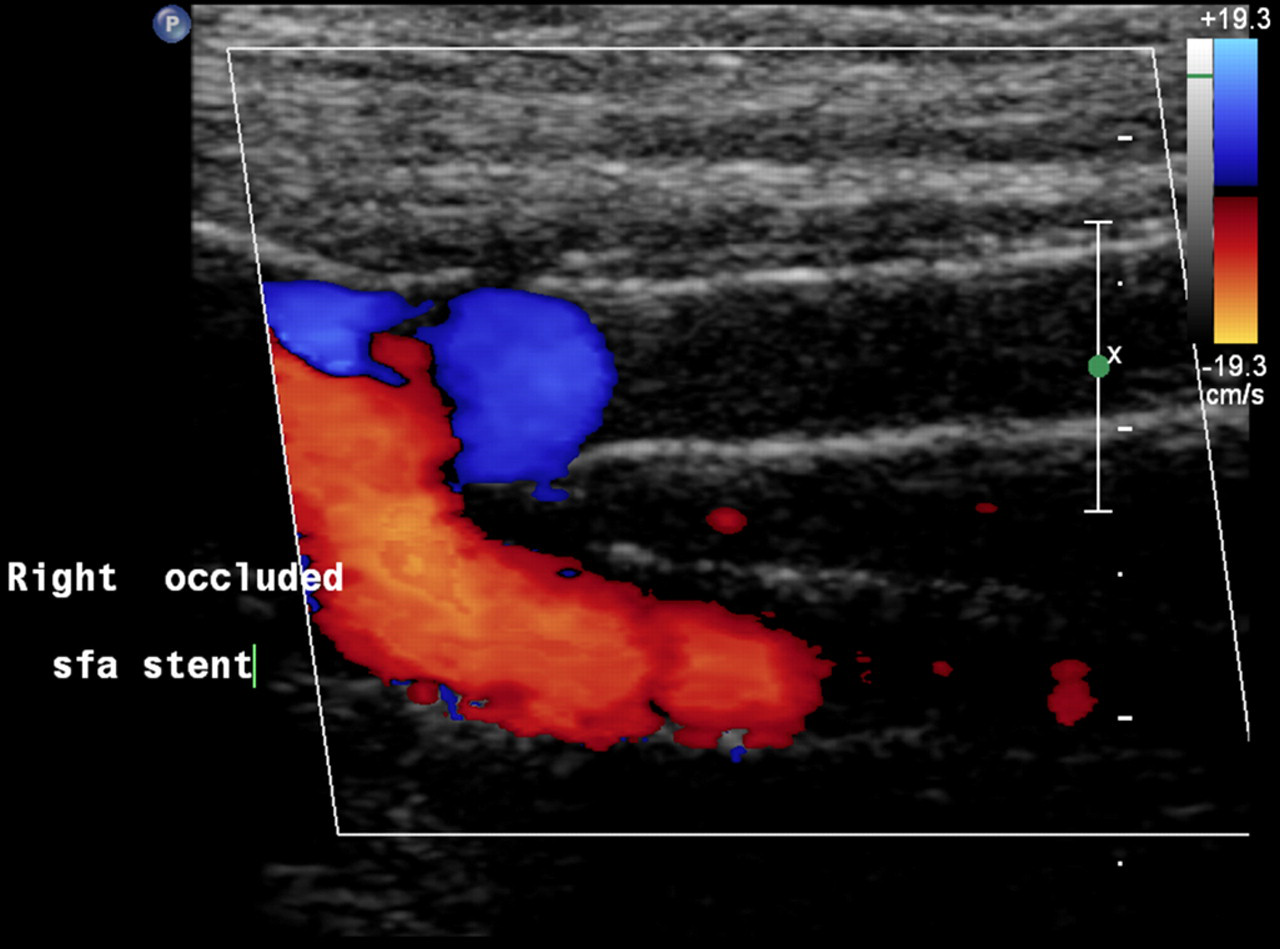

Two patients died of cardiac complications on the same admission, but unrelated to the stent procedure.
These results give an overall primary patency rate of 49% with an assisted primary patency rate of 76% at one year.
Discussion
Although digital subtraction angiography is the ‘gold standard’ for assessing stenosis within a stented peripheral artery, we have shown that ultrasound imaging and duplex assessment of narrowed areas, correlate well with subsequent angiographic findings.
The primary mode of stent failure is in-stent stenosis, which occurs in up to 40% of treated lesions. 7 Although patients with in-stent re-stenosis often do not present with recurrent symptoms, as evidenced by our study where 27% had ‘clinically silent’ stenoses, the implication exists that surveillance of these stented segments will result in higher assisted patency rates. 8
Recently, Baril et al. 8 described duplex criteria for the determination of in-stent stenosis after angioplasty and stenting of the SFA. As a department, we have used criteria from this study (>50% stenosis) to help guide both the sonographers and radiologists in determining optimal clinical management and to identify which patients will benefit from angiography and possible re-intervention, even if asymptomatic.
Early trials of nitinol stents in the femoropopliteal arterial segment reported stent fracture in 32%. Patency at 12 months was reduced from 84.3% to 41.1% in lesions with fractured stents, 9 although the direct relationship between stent fracture and patency remains controversial. With newer stent designs, the rate of fracture has reduced to approximately 2% at 12 months. 10 The RESILIENT trial 6 revealed a 4.1% stent fracture rate after 24 months and a study carried out by Ferreira et al., 11 also indicated that a nitinol stent can be implanted in the femoropopliteal arterial segment without high fracture rates for up to 4.8 years. However, not all stents in their series had a high resolution radiograph for evaluation, and this was recognized as a limitation.
In our department, SFA stenting is not followed up with radiographic imaging. This would be carried out only if it was likely to change management. Our interventional radiologists would consider restenting a fractured stent only if it was narrowed or symptomatic, which should therefore be detected by ultrasound or clinical follow-up. This information is effectively obtained when carrying out angiography, and to date there have been no patients symptomatic due to stent fractures within our department.
In our study, 27% of patients were found to have ‘clinically silent’ in-stent stenosis (>50%) on duplex ultrasound at one year and a further 10% had symptomatic in-stent stenosis or occlusion within the first year. These are similar results to those in stented groups of larger previously published studies (37% in the ABSOLUTE Trial 5 and 20% in the RESILIENT Trial 6 ).
One possible limitation of our study was the potential variability of stent technique and observer variability between the three different interventional radiologists in our department, although only two different stent types were used during the study and all cases were discussed at a vascular multidisciplinary meeting prior to and following intervention.
Of those patients in our study who had re-stenosis at one year, 82% had successful re-intervention, producing overall 72% assisted primary patency at one year. Monitoring patency is important to identify re-stenosis and to allow re-intervention when indicated, patency can then be optimized before the patient becomes symptomatic or the vessel becomes occluded, which would make re-intervention more difficult. In Ferreira et al.'s study, 11 the assisted primary-patency rates (endovascular re-intervention) were excellent at five years. In a further study by Saxon et al., 12 a secondary patency of 93% over five years was reported, and Kessel et al., 13 reported 12- month primary, primary assisted, and secondary patency rates of treated patients of 29%, 50% and 64% respectively. However this study was limited by the small sample size of just 20 patients.
Occlusions are known to be associated with markedly higher re-stenosis rates than a patent vessel with stenosis. 7 In our study, 64% had occlusive disease at the time of stenting. Of this subset, the primary patency rate at one year was 32%. Treatment of occlusions adds to the difficulty and complexity of SFA stenting when compared with treating a stenosis, thereby increasing complications. 14,15
Within our study one patient developed an asymptomatic occlusion. Initially, this patient had a long SFA occlusion (14 cm) who underwent angioplasty and stenting. There was no symptomatic improvement or decline following the procedure; however his routine 12-month scan confirmed a further occlusion. On this basis it may be presumed that the occlusion occurred relatively quickly.
We suspect that if an ultrasound scan had been carried out at six months, the eventual outcome is unlikely to have changed. Closer clinical scrutiny post-procedure, including regular ankle brachial pressure index (ABPI) measurements, may have diagnosed this occlusion at an earlier stage.
The specifics of disease, i.e. the length and severity, as suggested by Kessel et al. 13 and Schillinger et al., 5 predict poor outcomes of angioplasty or stenting. Retrospectively reviewing two of the patients who became symptomatic within the first year, an even more rigorous surveillance programme at three or six months is unlikely to have detected a stenosis prior to the occlusions as these look to have occurred at six and 53 days.
Diabetes mellitus is an important determinant of the risk of in-stent re-stenosis associated with stenting. 5 Diabetes is most likely to cause small vessel disease which in turn could affect the quality of the run-off vessels, ultimately leading to stenosis. 16 Although the run-off vessels were assessed by angiography during this study and angioplasty/stenting only performed in the presence of at least one patent crural vessel, incidence of diabetes was not documented and this may be a further limitation of our study.
Conclusion
Ideally, surveillance scans of the stented SFA at three , six and 12 months would help optimize patency before the patient became symptomatic; however, this would incur costs to both the patient and the hospital. Many centres do not perform any surveillance following stent placement, 17 relying on clinical symptoms alone to indicate in-stent stenosis. Instigating a sonographer-led service has enabled all patients to be followed up without impacting on the radiologists' workload in a busy vascular intervention unit.
Results from our study suggest that SFA stent follow-up at 12 months may be adequate in the treatment of SFA disease and that no clinically significant stenoses have been missed, thus ensuring very little change in terms of patient outcome. With good communication between imaging professionals and vascular surgeons to ensure that any symptomatic patients are assessed and imaged in a timely fashion, we will maintain routine surveillance on asymptomatic patients at 12 months.
DECLARATIONS